270 West 39th Street, STE 1701,
New York, NY 10018 1-800-810-3457
Vaccination vs ImmunizationUnderstanding the difference
IMMUNIZATION VS VACCINATION
Immunization means to make someone immune to something. Vaccination, by contrast, according to Dorland’s Medical Dictionary, just means to inject “a suspension of attenuated or killed microorganisms…administered for prevention…or treatment of infectious disease.”
Most people do not realize that when you receive a shot or a vaccine it does not mean you are immunized. Many people believe that once you are vaccinated you are completely protected. That belief is wrong.
The use of the word “immunization” instead of “vaccination” is everywhere. Most importantly, news outlets tell the public that immunization is the same as vaccination. However, there is a large difference between the two.
Vaccines contain a dead or live weakened germ that can cause a particular disease, like tetanus, or parts of a germ. When we are given a vaccine shot, our body immediately produces antibodies against the germ.
It is at this point that most believe the body’s defense mechanism kicks in and immunity will occur in the event that the said antigen gains entry again into the body but, this is not the case with all vaccines.
VACCINATION DOESN'T GUARANTEE IMMUNITY
Vaccination does not guarantee immunity. Natural immunity happens only after one recovers from the actual disease. During the disease, the microorganism usually has to pass through many of the body’s natural immune defense systems—in the nose, throat, lungs, digestive tract and lymph tissue—before it reaches the bloodstream.
As it does, the microorganism triggers many biological events that are essential in building true natural immunity. When a child gets a new disease, he may feel sick for several days, but, in the vast majority of cases, he will recover.
Defending what they believe is a misconception that the majority of people who get disease have been vaccinated, they state, “In fact it is true that in an outbreak those who have been vaccinated often outnumber those who have not – even with vaccines such as measles, which we know to be about 98% effective when used as recommended.”
“This is explained by two factors. No vaccine is 100% effective. Most routine childhood vaccines are effective for 85% to 95% of recipients.”
EVERYONE’S IMMUNE SYSTEM REACTS DIFFERENTLY
For reasons related to the individual, some will not develop immunity.
The second fact is that in a country such as the United States the people who have been vaccinated vastly outnumber those who have not. Here’s a hypothetical example of how these two factors work together.
The National Network of Immunization Information provides, “Although vaccines have very high effectiveness rates, they are not completely effective for 100% of the people who receive them. For example, a full series of measles vaccine will protect 99 of 100 children from measles and polio vaccine will protect 99 of 100 children from polio. This means when there is a disease outbreak, the very small number of people for whom the vaccine did not work may still be able to catch the disease. Because almost all of our children are immunized and only few are not, it can be the case that during an epidemic the majority of cases occur among children who were immunized. However, the fact remains that those who have not received the vaccine are much more likely to catch the disease.”
TYPES OF VACCINES
There are several different approaches that are used when vaccines are made. Each approach has its own way that it keeps the virus from sickening the recipient of the vaccine. When a company is developing a vaccine, they will have to choose which one of these methods works best to make the vaccine the most effective.
Here are the types of vaccines that are used:
WEAKENING VACCINES (LIVE ATTENUATED)
Some viruses reproduce thousands of times within the body. The bacteria invades the body and then it multiplies exponentially. This type of vaccine involves the introduction of the live virus into the body. While you may think that injecting a virus into the body will have harmful effects, the opposite holds true with these types of vaccines. The theory behind these vaccines is that they are intended to “educate” the body to defend itself from the virus. Once that occurs, the viruses will have difficulty reproducing within the body. Here, much of the work is done before the virus is injected into the body. The virus is grown outside of its normal environment. When that happens, it becomes a weakened form of itself. By the time that it is introduced to the body, it is unable to reproduce itself.
The advantages of live attenuated vaccines include:
They are relatively easy to create for the viruses that they protect against
They do not need to be taken more than once or twice
They help strengthen the immune system since they are very close to the actual virus
However, there are some disadvantages to this type of virus. They include:
Since they are weakened viruses, they can always re-strengthen and cause the sickness
They must be well-stored and refrigerated which makes them difficult to ship to certain places
Attenuated vaccines do not work well with bacterial viruses
Attenuated vaccines are used to immunize against the following diseases:
Measles, mumps, and rubella
Chickenpox
Smallpox
Yellow Fever
INACTIVATION VACCINES
Instead of introducing a weakened form of the virus into the body, this type of vaccine aims to completely stop the virus from reproducing. Usually, this type of vaccine will rely on a chemical or a pathogen to achieve that result. The body will continue to recognize the virus so it will keep producing the cells that will protect against the virus. The pathogen will still continue to exist, but it will not be able to replicate within the body.
The advantages of inactivation vaccines include:
No form of the disease will be produced by the body whatsoever. This includes even a milder form.
This is not a type of vaccine that cannot be given to those with weakened immune systems
However, unlike live attenuated vaccines, one or two injections will generally not be enough to provide lifetime protection against these diseases. In addition to the initial vaccination, several long-term booster shots will be necessary to continue to provide immunity against the diseases.
Types of diseases that are protected against by this type of vaccine include:
Polio
Rabies
Hepatitis A
SUBUNIT AND CONJUGATE VACCINES
Subunit vaccines use only a part of the virus in order to create the immunization. They take out only the essential part of the antigen in order to produce the vaccine and leave everything else. This will usually mean that a protein is used that resides on the surface of the virus. This type of vaccine is suitable for an instance where the body needs to protect against one specific part of the virus in order to protect against the entire disease. One of the advantages to this type of vaccine is that the body can give a targeted and focused response to the part of the germ that has been selected.
Conjugate vaccines use two different components instead of one. They use parts of the coats of bacteria. These parts are then linked to a protein. The combination of the coats of bacteria and the protein becomes the vaccine. It is the combination of the piece of bacteria and the carrier protein that gives the vaccine its effectiveness.
Some of the positive attributes of these types of vaccines include:
Those with weakened immune system and other health problems can receive the vaccine without fear of getting the disease
The immune response is strong and targeted
Those who receive this type of vaccine will likely require booster shots in order to receive continuous protection from the disease. In other words, recipients will not be able to have just one vaccination.
Some of the diseases that this type of vaccine protects against include:
Shingles
HPV
Hepatitis B
Meningococcal disease
Whooping cough
Pneumococcal disease
TOXOID VACCINES
Toxoid vaccines use the harmful thing that is produced by the disease called the toxin, inactivating it with a chemical and reintroducing it into the body. The inactivated toxin becomes the vaccine. As opposed to vaccinating against the entire germ, these vaccinate against the part of the germ that causes the disease. These types of vaccines are considered to be bacterial in nature because they contain the actual bacteria. In other words, when the inactivated toxins are introduced, they stimulate the production of antibodies to the toxin. However, they will not cause the disease itself to take root.
These vaccines can be given to people who have immune systems that are weakened or compromised. However, the amount of antibodies that is produced by the body declines over time with these types of vaccines. Thus, periodic booster shots are necessary to maintain the proper level of protection.
Some of the diseases treated by this type of vaccine include:
Tetanus Diphtheria
HOW ARE VACCINES ADMINISTERED?
There are several different ways that vaccines are administered. Most vaccines are administered through the form of an injection. However, advances in the medical field have diversified the means of delivery of new types of vaccines. Here are some means of administering vaccines through means other than an injection.
Nasal Spray - flu injections are given to patients through their nose as a mist.
Inhalant - There is a type of measles vaccine that is inhalable through the mouth.
Orally - Certain vaccines can given in tablet form.
Microneedle - Certain flu vaccines can shoot the substance into the body without the use of needles.
WHAT ARE THE TYPES OF IMMUNIZATION?
There are two different types of immunization. Each one has different features to it. The two types are active and passive immunizations. Below is some information on each of the two kinds of immunity.
ACTIVE IMMUNIZATION
The term "active immunization" characterizes how the body responds to receiving a vaccine. The vaccine stimulates the production of antibodies. Then, the antibodies will actively fight off the virus or the bacteria. The vaccine recipient will usually need a strong immune system in order to achieve the desired result. Active immunization cannot occur until the recipient has been exposed to the particular pathogen that is contained in the vaccine. The immunity is triggered by the exposure to the pathogen. Vaccines are considered to be a form of active immunization.
PASSIVE IMMUNIZATION
Passive immunity comes from the transfer of antibodies of an immune person to the body of a person who is not immune. This can happen naturally, such as when a mother passes immunity to a disease to the child through the fetus. It can also occur through a transfer in a substance such as immune globulin, which is given when protection from a certain disease is necessary. This protection occurs immediately, as opposed to active immunization, which takes time for the body to develop the necessary antibodies.
WHAT ARE THE DIFFERENCES BETWEEN ACTIVE AND PASSIVE IMMUNITY?
Active immunity takes some time to develop, usually as a response to receiving the vaccine. Passive immunity comes immediately upon transfer.
Passive immunity is not permanent and may last for a certain limited period of time. Active immunity is longer-lasting and is either permanent or lasts a long time until a subsequent booster shot is needed.
In passive immunity, the antibodies comes from outside the body. In active immunity, the antibodies come from within the body in response to the introduction of another substance.
There are three different possible reactions, or lack thereof, that people can experience when they have received immunizations and vaccinations. They are as follows:
No Side Effects - The majority of people who receive immunizations and vaccinations do not experience any side effects. Sometimes, there is soreness or redness at the site of injection, but nothing further. If there are minor side effects, it is often a sign that the vaccination is working insofar as the body is beginning to build up the resistance necessary to immunize against the disease.
Common Side Effects - While these side effects may be painful or temporarily debilitating, they are not much about which to be overly concerned. Among other things, these side effects consist of pain and itching at the injection site, dizziness, fever, nausea and a mild rash. Most often, these side effects pass after a period of time.
Serious Side Effects - In some instances, patients can have severe side effects based on how their bodies react to the vaccination. This could mean seizures, brain damage and in a worst-case scenario, death.
The most important thing is to know what to do when you or someone in your family begins to experience side effects from a vaccination. Here are several important considerations that span both legal and medical issues.
See a Medical Provider Immediately - If you believe that the side effects are anything more than common, it is essential to be seen by a healthcare provider immediately. From the obvious standpoint, adverse reactions to vaccination can endanger health both in the short and long terms. From a legal perspective, it is essential to document the complications that have been caused by an immunization.
Report the Side Effect - There is a Vaccine Adverse Event Reporting System that allows people to report any complications. Tracking any side effects is essential in order to both know about them and prevent widespread complications if possible.
Contact an Attorney - There is a National Vaccine Injury Compensation Program that exists for those who have suffered injury from receiving vaccines. This is a special court that has been set up which has its own rules and procedures. A claim must be filed in order to be eligible for compensation. An attorney who specializes in vaccine injuries will know the most effective way to file a claim for compensation.
COMMON SIDE EFFECTS
Pain, redness, tenderness or swelling at injection site
Fatigue
Headache
Itching at injection site
Nausea
Dizziness or fainting (most common in adolescents)
Fever
Mild rash
SERIOUS SIDE EFFECTS
Severe Allergic Reaction (Anaphylaxis)
Seizures
Brain Damage
Blood Disorders
Bowel Obstruction
Nerve Damage
Death
PEOPLE ASK: ...
VACCINE INJURY REPORTING
When one has sustained an injury as a result of being administered a vaccine, there is a different mechanism whereby one would receive compensation. Vaccines have both their own means of the reporting the injury as well as for filing a claim. This is not the same process that one would follow when they are injured by a medical device or medication.
WHY ARE VACCINES DIFFERENT THAN OTHER MEDICAL CLAIMS?
Congress passed the National Childhood Vaccine Injury Act in 1986 as a means of encouraging vaccine makers to produce their products while, at the same time, protecting patients from harm.
The intent behind the statute was to keep manufacturers from having to face litigation from the products that they sold.
On the other side, Congress also wanted to encourage people to be vaccinated by ensuring that they could be compensated for any injuries that they suffered.
HOW ARE VACCINE INJURIES REPORTED?
While the FDA has its own adverse event reporting database, the Centers for Disease Control, in tandem with the FDA, has its own Vaccine Adverse Event Reporting System for vaccine injuries. VAERS exists to serve as a repository for information about vaccine related injuries that can be reported to the database by anyone. There are several steps that one should take in order to report a vaccine injury to VAERS.
Contact healthcare provider - The first person to inform of an injury is the physician
Report the injury - Patients can submit an online report to VAERS
Update VAERS - If there are medical records pertaining to treatment, they should be uploaded into VAERS.
VAERS is helpful to track various metrics that relate to vaccines. Among the uses of VAERS are:
It helps to detect any trends in injuries
Allows people to track the safety of new vaccines
Gives transparency to adverse events for new vaccinations
Can identify any patient risk factors for certain vaccine injuries
THE NATIONAL VACCINE INJURY COMPENSATION PROGRAM
The VICP is the fund that allows those who have suffered vaccine-related injuries to receive compensation for their injuries. The main difference between vaccines and drugs is that, with regard to the VICP, the manufacturers are not paying out the settlement. That is because the VICP is intended to shield them from liability in order to encourage them to enter and stay in what is a critical field. The VICP was initially established because there was a scare related to a certain vaccine in the early 1980s that resulted in a threat to the vaccine supply when vaccine makers lost several large lawsuits.
The VICP is funded by a fee that is assessed by the federal government on the sale of every single childhood vaccination. The fees are then placed in the fund which is used to pay out claims as they are filed. This means that patients end up funding the settlements through the vaccines that are purchased.
There is a special mechanism for the VICP that must be followed in order to receive compensation. The process is started by filing a petition with the United States Court of Federal Claims (COFC), which has exclusive jurisdiction over vaccination cases. COFC has Special Masters whose job it is to decide these claims. Before the Special Master issues a decision, the Department of Health and Human Services will make their own recommendation. Then, the Department of Justice develops a report that includes a medical recommendation and legal analysis. After that, the Special Master may hold a hearing and decide the issue of compensation. The petitioner has the right to appeal the Special Master's decision.
It is best to hire an attorney to help with drafting the petition since the case will likely be decided initially on the basis of the petition and any hearing that the Special Master may hold. Given the scientific complexity of vaccines and their injuries, an attorney may best be able to present a case.
Here are the immunizations that may be recommended based on the immunization history and the answers you entered into the Rite Aid immunization Evaluation Questionnaire. This should be printed out and discussed with your Rite Aid pharmacist or health care provider before any immunizations are given.
Recommendations:
Shingles
Shingles vaccine is recommended to be administered. This immunization can be administered at your local Rite Aid.**
Flu
Flu vaccine is recommended to be administered. This immunization can be administered at your local Rite Aid.**
Diph/Tetanus/Pertussis
Diph/Tetanus/Pertussis vaccine is recommended to be administered. This immunization can be administered at your local Rite Aid.**
Pneumo/Prevnar
Pneumo/Prevnar vaccine is recommended to be administered. This immunization can be administered at your local Rite Aid.**
Have questions about insurance coverage or pricing?
Please contact your local Rite Aid pharmacist. Click here to locate a store nearest you. :: Click here for more information on diseases that can be immunized against.
*IMPORTANT: Only immunizations that may be required in the next 12 months are reported above. All answers are completely confidential, will not be stored and are not associated with your name when results are printed. The recommendations you will receive are not substitute for medical consultation or medical advice. All recommendations should be reviewed with a certified immunizing pharmacist or a health provider before any immunizations are given.
**Certain vaccinations may not be available in all locations. The availability of vaccines may depend upon state law. Age restrictions may vary by state. Please contact your Rite Aid Pharmacy to learn more.
Please note: All answers are completely confidential, will not be stored and are not associated with your name when results are printed.
Insurance Card: ________________ < MEDICARE
ID: ___________________
Group: ______________ I do not have insurance 1-2021 Identification must be provided for COVID Vaccine
Driver's License State____ #_____________
State ID State____ #_____________
I do not have ID
Screening Questionnaire and Consent Form Patient Information: (Patient to complete)
Patient Name: ____________________________
Date of Birth: _________
Age: _____
Phone#: ___________________
Address: ________________________________
City: ___________________________
State: ____
Zip: ____________
Email Address:_____________________________________________________________________________________
Gender: M or F Which vaccine(s) would you like to receive today?___________________________________________ Ethnicity: [ https://grants.nih.gov/grants/guide/notice-files/not-od-15-089.html ]
Hispanic or Latino (1);
Not Hispanic or Latino (2);
Unknown (3)
Race:
Black or African American (1);
White (2);
Asian (3);
American Indian/Alaska Native (4);
Native Hawaiian/Other Pacific Islander (5);
Unknown(6)
Medical Conditions: ___________________________________________ < SAH@MCA Stroke survivor
Enter Weight if less than 110 lbs.: __________
**FOR EMERGENCY USE ONLY** Primary Care Physician (PCP): _________________________________ Dr. Polina Sadikov, MD Dr. Phone: _____________________________ < (937) 832-1500
PCP address- City ________________________________________ State______Zip Code _______________________ ( Address: 9000 N Main St #300, Dayton, OH 45415 )
I authorize the pharmacist to send copies of my vaccine documents to my primary care provider. Yes No
Failure to select one of these boxes will result in the vaccine documents being sent to my primary care provider, if known, as state laws & regulations require for my state.
The following questions will help us determine which vaccines may be given today. If a question is not clear, please ask your pharmacist to explain it.
Yes, No, Don’t Know
1. Are you sick today? ( define "sick" )
2. Do you have a long term health problem with heart disease, kidney disease, metabolic disorder (e.g. diabetes), anemia or other blood disorders?
3. Do you have a long term health problem with lung disease or asthma?
4. Do you smoke?
5. Do you have allergies to:
a. medications,
b. food (i.e. eggs),
c. latex
or any d. vaccine component [ https://vaccine-safety-training.org/vaccine-components.html ]
(e.g. neomycin, formaldehyde, gentamicin, thimerosal, bovine protein, phenol, polymyxin, gelatin, baker’s yeast or yeast )?
6. Have you received any vaccinations in the past 4 weeks?
7. Have you ever had a serious reaction after receiving a vaccination?
8. Do you have a neurological disorder such as seizures or other disorders that affect the brain or have had a disorder that resulted from a vaccine (e.g. Guillain-Barre Syndrome)? ( stroke? survivor )
9. Do you have cancer, leukemia, AIDS, or any other immune system problem?
10. (in some circumstances you may be referred to your physician)
11. Do you take prednisone, other steroids, or anticancer drugs, or have you had radiation treatments?
12. During the past year, have you received a transfusion of blood or blood products, including antibodies?
13. Are you a parent, family member, or caregiver to a new born infant?
14. For women: Are you pregnant or could you become pregnant in the next three months?
I (Susan - a retired Technical Writer )authorize the release of any medical or other information with respect to this vaccine to my healthcare providers, Medicare, Medicaid or other third party payer as needed and request payment of authorized benefits to be made on my behalf to Rite Aid.
- I acknowledge that if my insurance does not cover the cost of administering the vaccine at the pharmacy, then payment must be made at the time of the administration of the vaccine. [ https://pubmed.ncbi.nlm.nih.gov/25166292/ ]
- I acknowledge that my vaccination record may be shared with federal or state or city agencies for registry reporting.
- I acknowledge that the pharmacist recommends that vaccinated patients should remain in the waiting area, for 15 minutes, after the administration of the immunization.
- I acknowledge receipt of Rite Aid’s Notice of Privacy Practices for Protected Health Information.
- I acknowledge that the administration of an immunization or vaccine does not substitute for an annual check-up with the patient’s primary care physician.
- For CA: I acknowledge that Rite-Aid intends to share my vaccination record with the California Immunization Registry (CAIR) and that I have reviewed the ‘CAIR Immunization Notice to Patients and Parents’ attached to this form.
- For CA: I acknowledge that if I do not want my immunization information shared with other CAIR users, I must complete and submit to CAIR a “Decline or Start Sharing/Information Request Form” obtained either from the pharmacy or downloaded from the CAIR website ( http://cairweb.org/cair-forms/ ).
- I certify my receipt of the services covered by this claim. I request that payment be made on my behalf. I authorize the holder to release medical information about me to any party involved in payment or their agents.
- I have read, or have had read to me the Vaccination Information Sheet (VIS) regarding the vaccine(s). I have had the opportunity to ask questions that were answered to my satisfaction and understand the benefits and risks of the vaccine(s).
I consent to, or give consent for, the administration of the vaccine(s).
I fully release and discharge Rite Aid Corporation, its affiliates, officers, directors, and employees from any liability for illness, injury, loss, or damage which may result there from.
[ "COVID" "VACCINE" IF YOU GET VERY SICK - AND REQUIRE HOSPITAL CARE - WHO PAYS THE BILL? ]
Jonathan Perez of Hoover, Ala., walking his dog, Meat Mountain. BOB MILLER FOR THE WALL STREET JOURNAL
Who Pays for Covid-19 Medical Care? That Depends on How (or if) You Are Insured
Pandemic has put a spotlight on the vast differences in affordability of health care across the country
By
PRINT
TEXT
merica, bills for Covid-19 treatment are coming due, and some patients are paying large out-of-pocket fees despite a federal safety net set up to help them avoid such financial surprises.
Early in the coronavirus pandemic, Congress formed an emergency system to ensure free testing for the virus and to help uninsured Americans avoid big hospital bills for Covid-19 treatment. At the same time, most large insurance companies waived cost-sharing agreements for Covid-19 patients, limiting out-of-pocket costs for holders of private health insurance.
The result, nine months into the pandemic, is a robust system to keep patients from receiving large “surprise bills” that result in major financial hardships, health-policy experts say.
But as many bills arrive, some patients, such as Medicare beneficiaries who don’t carry supplemental insurance, are falling through the cracks. And the uninsured are required to seek financial assistance and sometimes fill out labyrinthine paperwork to cover their bills, a tall task for many patients still suffering from the illness’s long-term effects.
WSJ NEWSLETTERSome Covid-19 Survivors Grapple With Large Medical Bills
While the federal government and health-care industry have worked to help Americans avoid costs associated with Covid-19 testing, some patients can be subject to high out-of-pocket costs for treatment, long after leaving the hospital.
Photo: Krystle Bodine and Drew Harris
“There’s a lot of confusion, and a lot of patients are scrambling,” says Jack Hoadley, a researcher at Georgetown University’s Health Policy Institute who has studied billing. “But what they’ve tried to create is a sort of patchwork universal health-care system for this one disease.”
The Wall Street Journal interviewed dozens of Covid-19 patients and identified four key groups that, based on their coverage status, experience the financial ramifications of infection in different ways.
Clutch Funding: The Uninsured
Jonathan Perez got sick at the tail-end of June. A 31-year-old Marine veteran who lives in Hoover, Ala., Mr. Perez had recently been laid off from his job as an office administrator for a nonprofit organization. Like nearly 28 million other Americans, he had no health insurance. One Monday morning, he started feeling a fever, body aches and chills. He tested positive for Covid-19 and spent a week at Shelby Baptist Medical Center in Birmingham, breathing oxygen from a tank. After a chest X-ray, a doctor told him, “A 31-year-old should not have this” level of lung damage, he says. Now back home, he has been walking his dogs three times a day to regain his wind.
Jonathan Perez had out-of-pocket costs of $876 for follow-up care and a chest X-ray.
PHOTO: BOB MILLER FOR THE WALL STREET JOURNAL
Mr. Perez says he applied for financial assistance through the hospital’s billing department, and was told the costs, which totaled between $50,000 and $55,000, would be covered by funds administered under the Cares Act, Congress’s emergency law that allocated $175 billion to providers to cover treatment costs for the uninsured. He received bills for follow-up care and a chest X-ray that weren’t done in the hospital, resulting in out-of-pocket costs of $876. A friend set up a GoFundMe campaign while he was in the hospital to help cover these costs.
Mr. Perez says he is thankful for the federal assistance. “I just figured that I wouldn’t get the virus as hard as other people.…It would be great if everyone, regardless of their situation, could get their bills paid.” Mr. Perez says even if he would have had to pay $100,000 or more, and became stuck in debt, it would have been worth it. “You only get one life,” he says.
Vulnerable: Some Medicare Beneficiaries
The six million Americans who are covered by Medicare but who don’t have supplementary insurance plans to cover cost-sharing, copayments and prescriptions “are the people who are most at risk of catastrophic health expenses,” says Tricia Neuman of the Kaiser Family Foundation.
Medicare, the government health plan that covers seniors and the disabled, doesn’t have out-of-pocket spending limits and hasn’t suspended its 20% cost-sharing for Covid-19 treatments.
Dawn Christensen’s family is getting by on about $3,000 a month in unemployment and disability payments.
PHOTO: DAWN CHRISTENSEN
Before the pandemic, Dawn Christensen, 52 years old, and her husband lived comfortably in Suffern, N.Y., on a household income of about $85,000. She taught wellness classes to senior citizens; he was an assistant manager at a Hilton property in New York City. Their two sons, ages 6 and 15, attended local Catholic schools.
The new coronavirus began attacking Ms. Christensen’s lungs in March. She visited the emergency room once, had an echocardiogram and was prescribed steroids, beta blockers, antibiotics and anti-inflammatory medications.
Her husband lost his job in July, and Ms. Christensen still doesn’t feel well enough to go back to work. The family is getting by on about $3,000 a month in unemployment and disability payments. She has had to pull her younger son from the Catholic school because the tuition was too expensive.
Because Ms. Christensen suffers from Ehlers-Danlos syndrome, a rare connective-tissue disease, she has been eligible for Medicare since 1999. In recent years, though, she hasn’t been able to afford supplemental insurance, which most Medicare recipients use to cover excess costs.
Her bills for treatment related to Covid-19 have totaled $9,500, and without gap coverage, her out-of-pocket portion has been more than $4,000 so far. She doesn’t have prescription medicine coverage under Medicare’s part D program and says she has been denied enrollment until the sign-up period begins in October. Her household income is too high for her to qualify for Medicaid.
The Centers for Medicare and Medicaid Services, which regulates the two public insurance programs, didn’t respond to requests for comment.
“This difficulty with not having supplemental insurance and the costs of prescriptions has been a major eye opener,” Ms. Christensen says. “Financially, we’re increasingly strapped.”
Traditional Medicare plans “don’t have some of the protections we think of as being more common in modern forms of insurance,” says Caitlin Donovan, a senior director at the National Patient Advocacy Foundation.
“The problems that are arising related to Covid-19 are not different in kind than the problems that exist all the time,” says Casey Schwarz, senior counsel at the Medicare Rights Center. “They’re just hitting more people at the same time.”
Covered: Low-Income Medicaid Holders
In theory, patients who have insurance through Medicaid, the government health insurance program for 72.5 million low-income Americans, shouldn’t be required to pay anything for Covid-19 treatment, says Ms. Donovan.
“The health-care system worked the way it was supposed to for Medicaid patients, but a lot of them have lost their jobs,” Ms. Donovan says. “For them, it’s more of a general safety-net issue.”
Kaisha Buchanan, a 29-year-old preschool teacher in Flint, Mich., went to the ER in May after developing problems breathing. She tested positive for Covid-19, and other tests showed problems with her heart, blood pressure and kidneys.
Kaisha Buchanan is the sole provider for her 5-year-old son, Kal-El Buchanan.
PHOTO: KAISHA BUCHANAN
Ms. Buchanan earns about $18,000 a year and is the sole provider for her 5-year-old son. She also suffers from type-2 diabetes and hypertension and has been on Medicaid for about three years.
“For the most part I just got poked and moved around and had my blood pressure taken. The doctors never really explained what was going on,” Ms. Buchanan says.
She was discharged and called back to work by her employer on June 15, before she had fully recovered from the infection and while still having respiratory problems. Within weeks, she received a letter saying she didn’t owe anything for her treatment.
Nearby Oakland County, outside of Detroit, saw a surge of cases starting in early April. There, the pandemic has led to 20,392 new Medicaid enrollments—an increase of 11%—in the first seven months of 2020, says Debbie Brinson, chief executive of Honor Community Health, a clinic that serves low-income patients in Pontiac, Mich. Some uninsured people who became ill with the virus received help enrolling in the program from health-care providers. Others got on Medicaid after losing a job and seeing their income fall.
“Medicaid in the midst of a pandemic is so, so important,” Ms. Brinson says. “These patients having access to Medicaid makes sure that the whole system doesn’t collapse because of the high costs providers are seeing.”
Mostly Covered: Private Insurance Holders
In early May, Michelle Vernezze, a 43-year-old nurse from Bristol, Wis., woke up with a fever, sore throat, dry cough and body aches. The next day, she noticed her urine was the color of Coca-Cola, which she recognized from her work at an internal-medicine clinic as a potential sign of kidney failure.
Her husband, Ron Vernezze, drove her to the Aurora Medical Center in nearby Kenosha. She has no memory of the 25 days that followed.
STAY INFORMED
Get a coronavirus briefing six days a week, and a weekly Health newsletter once the crisis abates: Sign up here.
<<< >>> Michelle Vernezze was put into an induced coma and attached to a ventilator for 16 days.
PHOTO: MICHELLE VERNEZZE
After testing positive for Covid-19, she developed a secondary bacterial infection that was attacking her lungs, kidneys, heart, pancreas and immune system, driving her white blood cell count to critically low levels and causing her tonsils to hemorrhage. She was put into an induced coma and attached to a ventilator for 16 days, spent 30 days in intensive care and received three blood transfusions. She later spent weeks hooked up to a dialysis machine for 24 hours a day. She was hospitalized for 52 days in total.
But when it comes to the bills, Ms. Vernezze, a mother of four who has spent her whole life in southeastern Wisconsin, considers herself one of the lucky ones.
Her encounter with coronavirus cost more than $ 836,000.00
Her total out-of-pocket costs so far: $602.66 in copayments to see an infectious-disease specialist and for an echocardiogram. Her insurance provider is covering the rest. About two-thirds of Americans under the age of 65 have private insurance through an employer. “We’ve barely had to pay a dime,” Ms. Vernezze says, which has allowed her to devote most of her energy to getting better. “When I look at the bill, I think, well, they saved my life. I think that’s worth it. Even just being able to walk is a blessing.” America’s Health Insurance Plans, an industry group, estimates that costs for insurers for Covid-19 treatment will total between $30 billion and $547 billion over two years.
Corrections & Amplifications --- Dawn Christensen’s family receives about $3,000 a month in unemployment and disability payments. An earlier version of this article and a photo caption incorrectly said $4,400 a month. (Corrected on Sept. 15.)
Appeared in the September 15, 2020, print edition as 'Virus Bills Highlight Coverage Disparities.' ..."
Patient Signature or legal guardian signature __________________________________________________________
Today’s Date (mm/dd/yy): ______/______/______
If legal guardian print name _________________________________________________________________________ PHARMACY USE ONLY
Lot #______________________________
Lot #_______________________________
Exp. Date _________________________
Exp. Date___________________________
Site RA or LA- Circle One Site RA or LA- Circle One Clinic
– Yes No Signature of pharmacist who administered Vaccine(s) and provided VIS to patient: __________________________________________
License #: ____________
NPI #: ______________
Date: _________
Signature of Certified Immunizing Technician or Intern who administered Vaccine(s): ________________________________________
Insurance Card: ________________ ID: ___________________ Group: ______________ I do not have insurance 1-2021 Identification must be provided for COVID Vaccine Driver's License State____ #_____________ State ID State____ #_____________ I do not have ID Screening Questionnaire and Consent Form Patient Information: (Patient to complete) Patient Name: ____________________________Date of Birth: _________ Age: _____ Phone#: ___________________ Address: ________________________________ City: ___________________________ State: ____ Zip: ____________ Email Address:_____________________________________________________________________________________ Gender: M or F Which vaccine(s) would you like to receive today?___________________________________________ Ethnicity: Hispanic or Latino (1); Not Hispanic or Latino (2); Unknown (3) Race: Black or African American (1); White (2); Asian (3); American Indian/Alaska Native (4); Native Hawaiian/Other Pacific Islander (5); Unknown(6) Medical Conditions: ___________________________________________ Enter Weight if less than 110 lbs.: __________ **FOR EMERGENCY USE ONLY** Primary Care Physician (PCP): _________________________________ Dr. Phone: _____________________________ PCP address- City ________________________________________ State______Zip Code _______________________ I authorize the pharmacist to send copies of my vaccine documents to my primary care provider. Yes No Failure to select one of these boxes will result in the vaccine documents being sent to my primary care provider, if known, as state laws & regulations require for my state. The following questions will help us determine which vaccines may be given today. If a question is not clear, please ask your pharmacist to explain it. Yes No Don’t Know Are you sick today? Do you have a long term health problem with heart disease, kidney disease, metabolic disorder (e.g. diabetes), anemia or other blood disorders? Do you have a long term health problem with lung disease or asthma? Do you smoke? Do you have allergies to medications, food (i.e. eggs), latex or any vaccine component (e.g. neomycin, formaldehyde, gentamicin, thimerosal, bovine protein, phenol, polymyxin, gelatin, baker’s yeast or yeast)? Have you received any vaccinations in the past 4 weeks? Have you ever had a serious reaction after receiving a vaccination? Do you have a neurological disorder such as seizures or other disorders that affect the brain or have had a disorder that resulted from a vaccine (e.g. Guillain-Barre Syndrome)? Do you have cancer, leukemia, AIDS, or any other immune system problem? (in some circumstances you may be referred to your physician) Do you take prednisone, other steroids, or anticancer drugs, or have you had radiation treatments? During the past year, have you received a transfusion of blood or blood products, including antibodies? Are you a parent, family member, or caregiver to a new born infant? For women: Are you pregnant or could you become pregnant in the next three months? Did you bring your Immunization Record Card with you? Are you currently enrolled in one of our medication adherence programs at Rite Aid (OneTrip Refill, Automated Courtesy Refills, or Rx Messaging- Text, Email, Phone)? Have you had the following vaccines: Yes No Don’t Know Pneumococcal Vaccine-- *you may need two different pneumococcal shots* Shingles Vaccine Whooping Cough (Tdap) Vaccine I authorize the release of any medical or other information with respect to this vaccine to my healthcare providers, Medicare, Medicaid or other third party payer as needed and request payment of authorized benefits to be made on my behalf to Rite Aid. - I acknowledge that if my insurance does not cover the cost of administering the vaccine at the pharmacy, then payment must be made at the time of the administration of the vaccine. - I acknowledge that my vaccination record may be shared with federal or state or city agencies for registry reporting. - I acknowledge that the pharmacist recommends that vaccinated patients should remain in the waiting area, for 15 minutes, after the administration of the immunization. - I acknowledge receipt of Rite Aid’s Notice of Privacy Practices for Protected Health Information. - I acknowledge that the administration of an immunization or vaccine does not substitute for an annual check-up with the patient’s primary care physician. - For CA: I acknowledge that Rite-Aid intends to share my vaccination record with the California Immunization Registry (CAIR) and that I have reviewed the ‘CAIR Immunization Notice to Patients and Parents’ attached to this form. - For CA: I acknowledge that if I do not want my immunization information shared with other CAIR users, I must complete and submit to CAIR a “Decline or Start Sharing/Information Request Form” obtained either from the pharmacy or downloaded from the CAIR website (http://cairweb.org/cair-forms/). - I certify my receipt of the services covered by this claim. I request that payment be made on my behalf. I authorize the holder to release medical information about me to any party involved in payment or their agents. - I have read, or have had read to me the Vaccination Information Sheet (VIS) regarding the vaccine(s). I have had the opportunity to ask questions that were answered to my satisfaction and understand the benefits and risks of the vaccine(s). I consent to, or give consent for, the administration of the vaccine(s). I fully release and discharge Rite Aid Corporation, its affiliates, officers, directors, and employees from any liability for illness, injury, loss, or damage which may result there from. Patient Signature or legal guardian signature __________________________________________________________ Today’s Date (mm/dd/yy): ______/______/______ If legal guardian print name _________________________________________________________________________ PHARMACY USE ONLY Lot #______________________________ Lot #_______________________________ Exp. Date _________________________ Exp. Date___________________________ Site RA or LA- Circle One Site RA or LA- Circle One Clinic – Yes No Signature of pharmacist who administered Vaccine(s) and provided VIS to patient: __________________________________________ License #: ____________ NPI #: ______________ Date: _________ Signature of Certified Immunizing Technician or Intern who administered Vaccine(s): ________________________________________ Place RX Label Here Place RX Label Here o Influenza Injectable o Pneumococcal o Hepatitis B o HPV o Varicella o IPV: o Meningococcal o Td o Hepatitis A o MMR o DTaP o Zoster (Shingles) o Tdap o Hepatitis A & B o Other: o Influenza Injectable o Pneumococcal o Hepatitis B o HPV o Varicella o IPV: o Meningococcal o Td o Hepatitis A o MMR o DTaP o Zoster (Shingles) o Tdap o Hepatitis A & B o Other:
Rite Aid is committed to making our website accessible for all customers, including those with disabilities.
We will continue to enhance our digital properties to deliver accessible experiences.
If you experience difficulty accessing our website content, reach out to our Customer Care.
Please note that COVID-19 vaccine doses are allocated by state and local jurisdictions.
Rite Aid can only make appointments to administer the doses we receive. Please understand that our customer care and pharmacists cannot schedule appointments and do not have information about future appointments.
Checking our dedicated site (riteaid.com/covid19) and your state or local jurisdiction’s website remain your best resources for up-to-date information.
We are doing everything in our power to make the process as fast and efficient as possible.
Together, we can bring an end to this pandemic. Thank you for your understanding and cooperation.


 < Click "
< Click "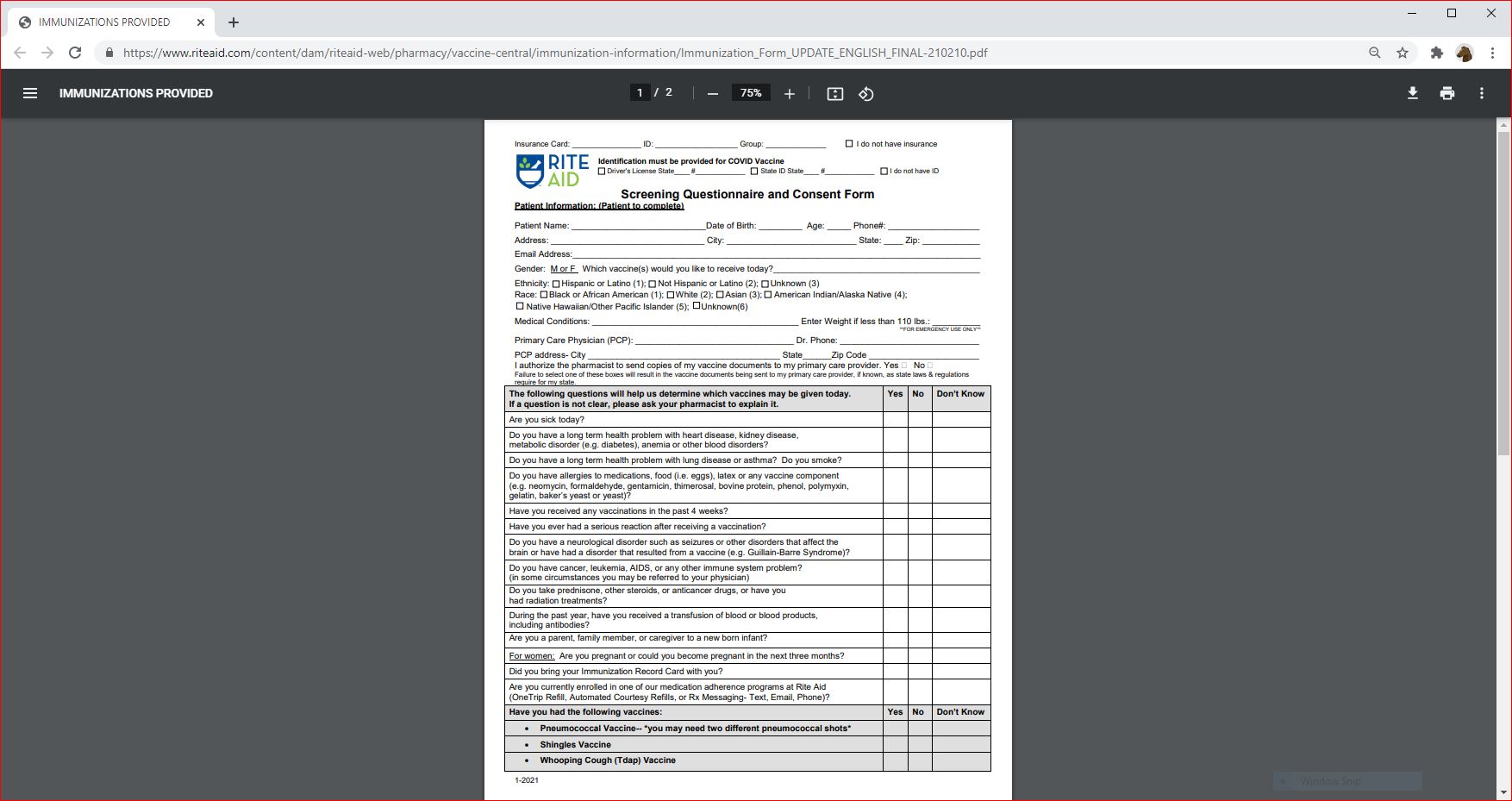




 hhhhhh
hhhhhh
