< HOME > 10 -19-2017 last update
HELLO! As the Health CARE debate "warms up" ...
On this page you will find hyperlinks to my related and copious research ( related to USA Health Care) and my NOTES.
 < I am Susan Marie [Cassady] - Neuhart. You are viewing the Universal Health Care RESEARCH page - of my "personal" web site.
< I am Susan Marie [Cassady] - Neuhart. You are viewing the Universal Health Care RESEARCH page - of my "personal" web site.
I am NOT a "candidate" for anything; nor, is any person - or company - paying me - for my stated views and comments. Although my Avatar is shown, I am a human being.
Based on my research, I have created a "BiLL" document for USA Health Care [ here ] - and, sent it to my USA Congressional Representatives. Also, our current USA President, Mr. Donald Trump.
ALL of them have responded - with form letters, email, telephone calls, etc. They all seem to use similar Political Management Software platforms also.
Which, this was predicted - by my Professors ( at OSU and UW ) - " heuristic and artificial intelligence based platforms" - in the 1980s. SEE "Sherlock"
 < the Camel is a beautiful creature ...
< the Camel is a beautiful creature ...
[ AND, designed by both evolutionary pressures & the environment - that it normally inhabits ] to live in rocky, drought-stricken areas (note the "humps").
MANY USA Government Programs emerge from Congressional Design Committees - appearing very similar to a Camel OR a Christmas Tree [ NOTE the "ornaments" ].  I am not subject to Congressional "Design Committee" pressures ( yet ) I respect the methods of the USA Congressional Research Service
I am not subject to Congressional "Design Committee" pressures ( yet ) I respect the methods of the USA Congressional Research Service
( http://www.loc.gov/crsinfo/about/ ) < NOTE, the dot "gov" URL
NOT to be confused with > http://congressionalresearch.org/ CRI
- thus, my USA Health Care bill idea - is NOT a Camel - OR - an ornamented object.
IT is - very simply - HOW it should be done.
I remain inspired by my USA Public college [ UWGB ] Professor's idealism & Harry Truman's spirit.
As a practical matter, WHAT does a USA Medical Professor get paid? ANSWER < Average At > Harvard Medical School
YES! You are welcome to look at it ( my research notes ), read it - and, use it (the information shown here)- FOR FREE - if you want to;
However, much of the information (shown here) MAY be "copyrighted" ( by its original Authors ); which I cite them - in each case.
So, please 1) be aware of this - 2) be respectful - AND 3) REQUEST PERMISSION - when it is warranted.
At the very least, please (try to) THANK! the original Authors. I provide contact information ( for them ) - as I am able.
KNOW THIS: I would not be able to assemble and create... but for, their efforts. (see HR676 )
YES - PNHP has published a new USA Health CARE document [43 pages] - in MAY of 2016 ( PDF )
<> I am reviewing this [ year 2016 ] document now ( to help USA Congress-people: Bernie Sanders, Mr. Conyers & Ms. Warren). My small "voluntary" assistance - to hyperlink the PNHP 's [2016] document's references
- is in progress - and, presented on my research page.
Very important! IN FACT! John Conyers or Elizabeth Warren - or their staffs - have never requested money or a donation (from me).

 hhhhhh
hhhhhh
< Avatar "Susan" by Hans ( THIS is Susan's personal web site: https://hansandcassady.org/ )
All content (at this site) is for my personal organization & mental enrichment only. Also, it makes it convenient for me to communicate. I DO NOT ACCEPT ANY MONEY FOR ANYTHING POSTED. Nor, do I plan to. Everybody has opinions - following are mine. If you - or your organization ( Democrats, Republicans or hypocrites of any kind ) - appear on my personal web site & you do not wish to - Please, send me a message - by using my Contact form.
[ THIS SITE BEST VIEWED WITH A "REAL", FULL-SIZED DESK MONITOR ]
Note: "Hans & Cassady, Inc." is no longer a USA business entity. Susan is retired - and, lovin' it. YES - I "volunteer" - as I am able - and, Hans (my husband) approves.
~ Building this HTML "web site" is an ongoing "experiment". ... See Stroke & Doctors in Table.
update 7-16-2017:: ReDEsign of my web site content now underway TABLE > Content& subjects (below) will be "hyperlinked" to individual HTML pages ( after re-organization )
ON USA HEALTH CARE: AS Proposed in 1989 - PDF ] < "A National Health Program for the United States: A Physicians' Proposal"
[ Review & Comments DONE ( on 1989 proposal) & "bug report" filed with PNHP ] link
NOTE: PNHP has published a new USA Health CARE document [43 pages] - in MAY of 2016 ( PDF ) <> I am reviewing this [ year 2016 ] document now ( to help USA Congress-people Mr. Conyers & Ms. Warren). My small "voluntary" assistance - to hyperlink the PNHP 's [2016] document's references - is in progress - and, presented on my research page.
http://www.pnhp.org/hr676cosponsors < Very helpful information! - related to local "activism" and HR676. ALSO
FROM the PNHP web site: "...What is Single Payer? " Single-payer national health insurance, also known as “Medicare for all,” is a system in which a single public or quasi-public agency organizes health care financing, but the delivery of care remains largely in private hands. Under a single-payer system, all residents of the U.S. would be covered for all medically necessary services, including doctor, hospital, preventive, long-term care, mental health, reproductive health care, dental, vision, prescription drug and medical supply costs. The program would be funded by the savings obtained from replacing today’s inefficient, profit-oriented, multiple insurance payers with a single streamlined, nonprofit, public payer, and by modest new taxes based on ability to pay. Premiums would disappear; 95 percent of all households would save money. Patients would no longer face financial barriers to care such as co-pays and deductibles, and would regain free choice of doctor and hospital. Doctors would regain autonomy over patient care. "
PDF <USA DOD’s use of MiLitary Standards and Specifications
[ This document PDF Answers WHY they do it - this way-in the USA Military. We "could" do it THIS way - also - in USA Health Care. my research page.
Bernie Sanders Bill ( PDF ) Mr. Bernie Sander's Plan ( " medicare for all" ) is NOT "Socialized Medicine" - as defined by Harry S. Truman (1945). My idea (above) - on the other hand - would make ALL USA Medical Professionals employees of the USA Government. Thus, by the definition of Harry S. Truman (1945)- my idea (my detailed plan) is "socialized medicine".
Mr. Sanders Bill (S.1804 - Medicare for All Act of 2017 - Introduced 09/13/2017 PDF ) encourages the sale of "Private Health Insurance" in the USA. See page 66 of the Bill PDF . My independent research ( presented here ) indicates the legal existence of any such "Health Insurance" product is inimical to the success of Socialized Medicine.
Moreover, Mr. Sander's Bill does not address the COST of Medical Professional services directly - or cap them - by law. Rather, his bill ( S 1804 PDF ) seeks to engender the support of organizations - literally hostile to the every day well-being of the average USA citizens - such as the AMA. With the result ( of S 1804 PDF) that USA Healthcare Professionals will continue to be paid far above what their international counter-parts are paid - for similar services - yet, USA Medical Professionals would typically work 4-day work weeks - and, be advised to implement (so-called) "patient management systems" - that treat USA citizens - who require medical care - as "objects" moving through the very Patient Management Systems ( the AMA supports the development of). The AMA sells PMS - as products - on the AMA web site). See the "Practice Management" tab of the AMA.
Mr. Sander's Bill does not seek to fundamentally change USA Medical Care. His bill (S 1804 PDF)seeks to preserve the status quo ( that, USA Medical Doctors are "special" - above and beyond other USA working professionals. For Example USA College Level Medical Professors... ) - and thus, the upward trajectory of USA cost of care will not change. Indeed, if Bernie's Bill [S 1804] is passed, costs will rise - as the USA Health Insurance, Medical Network Industry takes ever more control of methods and procedures - and, the implementation of USA Health Care. - Susan
FOR EXAMPLE: PREMIER Health PLAN Insurance : https://www.premierhealthplan.org/
Premier Health Plan offers 1) the Premier Health Advantage (HMO), 2) Premier Health Advantage Choice™ (HMO-POS), and 3) Premier Health Advantage VIP (HMO SNP) health insurance products.
Premier Health Plan has a Medicare contract and an Ohio Medicaid contract. Enrollment in Premier Health Advantage, Premier Health Advantage Choice, or Premier Health Advantage VIP depends on contract renewal.
This insurance plan is underwritten by Premier Health Insuring Corporation. Premier Health Insuring Corporation does business under the name Premier Health Plan.
Medicare evaluates plans based on a 5-star rating system. Star Ratings are calculated each year and may change from one year to the next. H3233_18_4026 Pending CMS Approval
NON-compliance [ PDF ] https://www.cms.gov/Medicare/Compliance-and-Audits/Part-C-and-Part-D-Compliance-and-Audits/Enforcement-Letters-Items/Premier-Health-CMP-09-18-17.html
Contact: Ms. Renee George, President - Premier Health Insuring Corporation, 110 North Main Street, Suite 1200 Dayton, OH 45402 Telephone: (937) 499-7441
NATIONAL HEALTH POLICY CONFERENCE 2018 > March 07 – 08, 2018 Washington, D.C. ( https://www.ahip.org/ahips-national-health-policy-conference-2017-faq/ )
Academy for Healthcare Management, America’s Health Insurance Plans, https://www.ahip.org/ahm-courses-and-designations/
Healthcare Financial Management Association. https://www.hfma.org/
11-12-2017
HEALTH CARE > "price fixing"
https://www.ftc.gov/tips-advice/competition-guidance/guide-antitrust-laws/dealings-competitors/price-fixing
A plain agreement among competitors to fix prices is almost always illegal, whether prices are fixed at a minimum, maximum, or within some range.
Illegal price fixing occurs whenever " two or more competitors agree to take actions that have the effect of raising, lowering or stabilizing the price of any product or service without any legitimate justification."
What is 'legitimate justification' - related to USA citizen pain&suffering :: compare to business justification AND profit motive.
[ Basically, in America (today) the Medical Doctors DO NOT compete for your business. Instead, the Medical Doctors are members of a "Network"; the purpose (of which) - it is - to set market prices [ "price fixing" ] - for health-related goods & services. Thus, the Health Care Insurance Industry bottom-line "take home" becomes ever larger. - Susan
Price-fixing schemes are often worked out in secret and can be hard to uncover, but an agreement can be discovered from "circumstantial" evidence. [ < THIS IS WHERE THE USA AMA COMES IN! ]
Contact Susan - or the USA-FTC officers - to help prove (that) this is what the USA Medical Industry is doing. Save copies of your health care related medical service invoices; AND, show them to the FTC officers.
" For example, if direct competitors have a pattern of unexplained identical contract terms or price behavior together with other factors (such as the lack of legitimate business explanation), unlawful price fixing may be the reason. Invitations to coordinate prices also can raise concerns, as when one competitor announces publicly that it is willing to end a price war if its rival is willing to do the same, and the terms are so specific that competitors may view this as an offer to set prices jointly."
https://en.wikipedia.org/wiki/Price_fixing
RESPONSE TO: < PDF includes MediCARE History SHORT REPLY submitted USA Ohio SENATOR : Rob Portman USA Ohio SENATOR : Sherrod Brown
Susan's Voting PRECINCT is "I" - Harrison TWP - Montgomery County, Ohio, USA.
An image of the USA "ballot" that Susan will cast: ( PDF )
If you "vote" - and, I hope that YOU will - Please be familiar with the issues & the candidates that you will requested to "cast" a vote on.
[Research Info for me and others ... https://www.voterfind.com/montgomeryoh/ballotlist.aspx < IF YOU LIVE IN MONTGOMERY COUNTY - OHIO - Click TO View and Find YOUR Ballot :: IF YOU ARE YES - AN OHIO RESIDENT - BUT, DO NOT LIVE IN MONTGOMERY COUNTY - OHIO - THEN,
YOU must learn your "locality": County? City? Town? etc. And, (then) START here: THE OHIO County Board of Elections: https://www.ohio.gov/government/localities/
OR https://www.sos.state.oh.us/elections/elections-officials/county-boards-of-elections-directory/
 To see BIGGER image (CLICK lINK) > http://www.mcboe.org/pdfmaps/1600.pdf?636444580729055809
To see BIGGER image (CLICK lINK) > http://www.mcboe.org/pdfmaps/1600.pdf?636444580729055809
< YES! Map [on file] at BOE at present NEEDS Bigger Labels. David, Linda, Mark & Deerek - WE are all working on this.
CONTACT: Montgomery County OHIO Board of Elections, 451 W. Third Street, Dayton, Ohio 45422 Phone:(937) 225-5656 email to:MCBOE@MCOHIO.ORG Their web site: www.mcboe.org
Comprehensive Health Program ( A BiLL to the USA CONGRESS ) - by HARRY S. TRUMAN - 33rd President of the United States of America :: 1945-harry-truman-calls-for national-health-insurance-program :: PBS Quote: "Almost as soon as the ... bill was announced, the …-powerful American Medical Association (AMA) capitalized on the nation’s paranoia over the threat of Communism and, despite Truman’s assertions to the contrary, attacked the bill as “socialized medicine.” SEE: wwwDOTpbsDOTorg forward slash” newshour “ program.
Posted 10-23-2017: Dear Ohio Senators: Brown and Portman, RE: “The Bipartisan Health Care Stabilization Act of 2017” < Google for details
Please STOP! this Congressional "BiLL sham" is (basically) designed to HELP Insurance Companies MAKE EVEN MORE MONEY!!
Please instead, show Mr. Trump > Susan's HealthCARE Idea that is shown (HERE) on my personal web site.
NOTE ( for Mr. Trump) that my inspiration is from Harry S. Truman (1945). AND, tell him that I am a "buckeye" !
The daughter of Milo Gerald CassADY. Thus, the niece of Pearl CassAdy. Pearl's son [Howard] won the Heisman Trophy - for OSU - in 1955.
I am just a senior USA citizen. AND, although I am willing to help him - with this Harry S. Truman "inspired" idea, I am still an Obama Girl.
The details of this breaking news story (RE: to Chuck Shumer) are posted and linked on my web site.
PRESS RELEASE - from USA Senator Lamar Alexander's Office > LINK URL: https://www.alexander.senate.gov/public/index.cfm/2017/10/group-of-24-senators-cosponsors-short-term-legislation-to-stabilize-premiums-access-to-insurance
"Touted by:" Chuck Shumer ( ? a DeMOcrat ?) [ PDF of story in New York Daily News ] [ "Touted by" Chuck Shumer ( ? a DeMOcrat ?) < link to NYD News article ]
This "BiLL" (currently NOT numbered is Authored by: Tennessee Republican Lamar Alexander AND Washington Democrat Patty Murray
Working TiTled as: “The Bipartisan Health Care Stabilization Act of 2017.”
The bill [ Full TEXT - Section Summary ] --- ( is not numbered at this writing) AND is CO-sponsored by: ONLY 12 Republican Senators Mike Rounds (R-S.D.),
Lindsey Graham (R-S.C.), John McCain (R-Ariz.), Bill Cassidy (R-La.), Susan Collins (R-Maine), Joni Ernst (R-Iowa), Lisa Murkowski (R-Alaska),
Charles Grassley (R-Iowa), Johnny Isakson (R-Georgia), Richard Burr (R-N.C.), and Bob Corker (R-Tenn.);
AND, 12 Democratic Senators Angus King (I-Maine), Jeanne Shaheen (D-N.H.), Joe Donnelly (D-Ind.), Amy Klobuchar (D-Minn.), Heidi Heitkamp (D-N.D.), Al Franken (D-Minn.),
Joe Manchin (D-W.Va.), Tom Carper (D-Del.), Tammy Baldwin (D-Wis.), Claire McCaskill (D-Mo.), and Maggie Hassan (D-N.H.)
[ AT THIS WRiTing, YOU! - MY Ohio Senators ARE not publicly shown - in support. ]
USA Senator - Rob Portman ( Ohio REP) Sherrod Brown is also my USA Ohio Senator...( Ohio DEM)
I will email "MESSAGE" my request to them: MESSAGE sent If you agree with ME - and, I hope that you do - Please also "message" your USA Senators.
Bernie Sanders Bill ( PDF ) Mr. Bernie Sander's Plan ( " medicare for all" ) is NOT "Socialized Medicine" - as defined by Harry S. Truman (1945). My idea (above) - on the other hand - would make ALL USA Medical Professionals employees of the USA Government. Thus, by the definition of Harry S. Truman (1945)- my idea (my detailed plan) is "socialized medicine".
Mr. Sanders Bill (S.1804 - Medicare for All Act of 2017 - Introduced 09/13/2017 PDF ) encourages the sale of "Private Health Insurance" in the USA. See page 66 of the Bill PDF . My independent research ( presented here ) indicates the legal existence of any such "Health Insurance" product is inimical to the success of Socialized Medicine.
Moreover, Mr. Sander's Bill does not address the COST of Medical Professional services directly - or cap them - by law. Rather, his bill ( S 1804 PDF ) seeks to engender the support of organizations - literally hostile to the every day well-being of the average USA citizens - such as the AMA. With the result ( of S 1804 PDF) that USA Healthcare Professionals will continue to be paid far above what their international counter-parts are paid - for similar services - yet, USA Medical Professionals would typically work 4-day work weeks - and, be advised to implement (so-called) "patient management systems" - that treat USA citizens - who require medical care - as "objects" moving through the very Patient Management Systems ( the AMA supports the development of). The AMA sells PMS - as products - on the AMA web site). See the "Practice Management" tab of the AMA.
Mr. Sander's Bill does not seek to fundamentally change USA Medical Care. His bill (S 1804 PDF)seeks to preserve the status quo ( that USA Medical Doctors are "special" - above and beyond other USA working professionals ) - and thus, the upward trajectory of USA cost of care will not change. Indeed, if his Bill [S 1804] is passed, costs will rise - as the USA Health Insurance, Medical Network Industry takes ever more control of methods and procedures - and, the implementation of USA Health Care. - Susan
http://www.nonprofitfacts.com/OH/Premier-Health-Partners.html < This is WHERE the money goes - when an Insurance NETwork runs the show.
11-12-2017
HEALTH CARE > "price fixing"
https://www.ftc.gov/tips-advice/competition-guidance/guide-antitrust-laws/dealings-competitors/price-fixing
A plain agreement among competitors to fix prices is almost always illegal, whether prices are fixed at a minimum, maximum, or within some range.
Illegal price fixing occurs whenever " two or more competitors agree to take actions that have the effect of raising, lowering or stabilizing the price of any product or service without any legitimate justification."
What is 'legitimate justification' - related to USA citizen pain&suffering :: compare to business justification AND profit motive.
[ Basically, in America (today) the Medical Doctors DO NOT compete for your business. Instead, the Medical Doctors are members of a "Network"; the purpose (of which) - it is - to set market prices [ "price fixing" ] - for health-related goods & services. Thus, the Health Care Insurance Industry bottom-line "take home" becomes ever larger. - Susan
Price-fixing schemes are often worked out in secret and can be hard to uncover, but an agreement can be discovered from "circumstantial" evidence. [ < THIS IS WHERE THE USA AMA COMES IN! ]
Contact Susan - or the USA-FTC officers - to help prove (that) this is what the USA Medical Industry is doing. Save copies of your health care related medical service invoices; AND, show them to the FTC officers.
" For example, if direct competitors have a pattern of unexplained identical contract terms or price behavior together with other factors (such as the lack of legitimate business explanation), unlawful price fixing may be the reason. Invitations to coordinate prices also can raise concerns, as when one competitor announces publicly that it is willing to end a price war if its rival is willing to do the same, and the terms are so specific that competitors may view this as an offer to set prices jointly."
https://en.wikipedia.org/wiki/Price_fixing
RESPONSE TO: < PDF includes MediCARE History SHORT REPLY submitted USA Ohio SENATOR : Rob Portman USA Ohio SENATOR : Sherrod Brown
Susan's Voting PRECINCT is "I" - Harrison TWP - Montgomery County, Ohio, USA.
An image of the USA "ballot" that Susan will cast: ( PDF )
If you "vote" - and, I hope that YOU will - Please be familiar with the issues & the candidates that you will requested to "cast" a vote on.
[Research Info for me and others ... https://www.voterfind.com/montgomeryoh/ballotlist.aspx < IF YOU LIVE IN MONTGOMERY COUNTY - OHIO - Click TO View and Find YOUR Ballot :: IF YOU ARE YES - AN OHIO RESIDENT - BUT, DO NOT LIVE IN MONTGOMERY COUNTY - OHIO - THEN,
YOU must learn your "locality": County? City? Town? etc. And, (then) START here: THE OHIO County Board of Elections: https://www.ohio.gov/government/localities/
OR https://www.sos.state.oh.us/elections/elections-officials/county-boards-of-elections-directory/
To see BIGGER image (CLICK lINK) > http://www.mcboe.org/pdfmaps/1600.pdf?636444580729055809
< YES! Map [on file] at BOE at present NEEDS Bigger Labels. David, Linda, Mark & Deerek - WE are all working on this.
CONTACT: Montgomery County OHIO Board of Elections, 451 W. Third Street, Dayton, Ohio 45422 Phone:(937) 225-5656 email to:MCBOE@MCOHIO.ORG Their web site: www.mcboe.org
Comprehensive Health Program ( A BiLL to the USA CONGRESS ) - by HARRY S. TRUMAN - 33rd President of the United States of America :: 1945-harry-truman-calls-for national-health-insurance-program :: PBS Quote: "Almost as soon as the ... bill was announced, the …-powerful American Medical Association (AMA) capitalized on the nation’s paranoia over the threat of Communism and, despite Truman’s assertions to the contrary, attacked the bill as “socialized medicine.” SEE: wwwDOTpbsDOTorg forward slash” newshour “ program.
Posted 10-23-2017: Dear Ohio Senators: Brown and Portman, RE: “The Bipartisan Health Care Stabilization Act of 2017” < Google for details
Please STOP! this Congressional "BiLL sham" is (basically) designed to HELP Insurance Companies MAKE EVEN MORE MONEY!!
Please instead, show Mr. Trump > Susan's HealthCARE Idea that is shown (HERE) on my personal web site.
NOTE ( for Mr. Trump) that my inspiration is from Harry S. Truman (1945). AND, tell him that I am a "buckeye" !
The daughter of Milo Gerald CassADY. Thus, the niece of Pearl CassAdy. Pearl's son [Howard] won the Heisman Trophy - for OSU - in 1955.
I am just a senior USA citizen. AND, although I am willing to help him - with this Harry S. Truman "inspired" idea, I am still an Obama Girl.
The details of this breaking news story (RE: to Chuck Shumer) are posted and linked on my web site.
PRESS RELEASE - from USA Senator Lamar Alexander's Office > LINK URL: https://www.alexander.senate.gov/public/index.cfm/2017/10/group-of-24-senators-cosponsors-short-term-legislation-to-stabilize-premiums-access-to-insurance
"Touted by:" Chuck Shumer ( ? a DeMOcrat ?) [ PDF of story in New York Daily News ] [ "Touted by" Chuck Shumer ( ? a DeMOcrat ?) < link to NYD News article ]
This "BiLL" (currently NOT numbered is Authored by: Tennessee Republican Lamar Alexander AND Washington Democrat Patty Murray
Working TiTled as: “The Bipartisan Health Care Stabilization Act of 2017.”
The bill [ Full TEXT - Section Summary ] --- ( is not numbered at this writing) AND is CO-sponsored by: ONLY 12 Republican Senators Mike Rounds (R-S.D.),
Lindsey Graham (R-S.C.), John McCain (R-Ariz.), Bill Cassidy (R-La.), Susan Collins (R-Maine), Joni Ernst (R-Iowa), Lisa Murkowski (R-Alaska),
Charles Grassley (R-Iowa), Johnny Isakson (R-Georgia), Richard Burr (R-N.C.), and Bob Corker (R-Tenn.);
AND, 12 Democratic Senators Angus King (I-Maine), Jeanne Shaheen (D-N.H.), Joe Donnelly (D-Ind.), Amy Klobuchar (D-Minn.), Heidi Heitkamp (D-N.D.), Al Franken (D-Minn.),
Joe Manchin (D-W.Va.), Tom Carper (D-Del.), Tammy Baldwin (D-Wis.), Claire McCaskill (D-Mo.), and Maggie Hassan (D-N.H.)
[ AT THIS WRiTing, YOU! - MY Ohio Senators ARE not publicly shown - in support. ]
USA Senator - Rob Portman ( Ohio REP) Sherrod Brown is also my USA Ohio Senator...( Ohio DEM)
I will email "MESSAGE" my request to them: MESSAGE sent If you agree with ME - and, I hope that you do - Please also "message" your USA Senators.
sssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssssss
To SEND me a message OR, ask me a question, Please - just use my Contact form ( click )
Please be aware: Shown above is my 1996 "avatar". My husband is (the) USA Digital Artist, Hans Neuhart. The photo (shown - at left) is me - before I had a stroke - in 2012. In fact, I am a senior - USA citizen [b.1954]; I am very happily married! I am a retired lady. I follow my doctor's instructions [ that include performing my YOGA poses every day]. I have had GREAT USA medical doctors! And, I consider myself "one of the lucky ones" ! That is, considering the state of USA Medical Care.
Hyperlinked RESEARCH & NOTES re: THE USA Health CARE System ( as envisioned by a USA citizen & voter - Susan)
“A long habit of not thinking a thing wrong, gives it a superficial appearance of being right, and raises at first a formidable outcry in defense of custom.
But the tumult soon subsides. Time makes more converts than reason.” Thomas Paine
And, so it goes with American Health Care - and, the CURRENT practice of American Health Care INSURANCE. [ which we - TOGETHER - will change ]
- Please, send me a message - by using my Contact form.
https://popularresistance.org/ < NOTE:Susan is NOT associated with this group. (Yet) I mention this because I link (to them) in my research below. "POPReSist" covered the release of the PNHP (2016-May) Proposal(below)
AS Proposed in 1989 - PDF ] < "A National Health Program for the United States: A Physicians' Proposal" ( NOTE:"[1989]...proposal was drafted by a 30-member 'Writing Committee'." - See paragraph just after references cited.)
HORSE built by committee = "camel" > Clearly, camels are beautiful ! > 
NOTE: PNHP published a new document - in MAY of 2016 ( the original PDF from the PNHP web site) < Please remember to THANK them - if you use this PDF *
" Beyond the Affordable Care Act: A Physicians’ Proposal for Single‐Payer Health Care Reform "
I am reviewing this recent [ year 2016 ] document now. [* Susan's PDF (of their 2016 "enCrypted" PDF document) - that has been UN-encrypted ]
No need to "THANK" me - just participate AND - VOTE!
(CAMEL ALERT! " This 2016 "proposal" was "drafted" by a 39 member working group..." see their PDF page 1. )
References : NOTE- the PNHP Year 2016 ( PDF )document does NOT have "live links" - for references. ARGH!, OhiO BUCKEYES ( of which I am one ) call what PNHP has done (thus far) "a-half-assed-help-ya." So, I have followed the PDF document "reference-section-bread-crumbs" - provided in their PDF "2016 "proposal" AND... - "live links" for the PNHP ( PDF ) document2016 - and, my best guesses - of what they were trying (maybe?) to cite - Follow: GOOD LUCK!
http://www.pnhp.org/hr676cosponsors < Very helpful information! - related to local "activism" and HR676. ALSO FROM the PNHP web site: "...What is Single Payer? " Single-payer national health insurance, also known as “Medicare for all,” is a system in which a single public or quasi-public agency organizes health care financing, but the delivery of care remains largely in private hands. Under a single-payer system, all residents of the U.S. would be covered for all medically necessary services, including doctor, hospital, preventive, long-term care, mental health, reproductive health care, dental, vision, prescription drug and medical supply costs. The program would be funded by the savings obtained from replacing today’s inefficient, profit-oriented, multiple insurance payers with a single streamlined, nonprofit, public payer, and by modest new taxes based on ability to pay. Premiums would disappear; 95 percent of all households would save money. Patients would no longer face financial barriers to care such as co-pays and deductibles, and would regain free choice of doctor and hospital. Doctors would regain autonomy over patient care. "
PDF <USA DOD’s use of MiLitary Standards and Specifications
[ This document PDF Answers WHY they do it - this way-in the USA Military. We "could" do it THIS way - also - in USA Health Care. my research page.
ALERT! The AMA document "AMA VISION ON HEALTH REFORM "- that I just "downloaded" is a sham - that ONLY (really) supports USA 'Health Insurance' companies - and, even more injustice!
Susan says: THE " AMA "IS Single-Payer Health Care's" ENEMY - (thus) "AMA" is "our"ENEMY!
Please become informed. Inform any Medical Professionals (that you know) - and VOTE! [ Politics RNC & DNC ]
Also - Let Us "protest" [if needed] - real nice & peaceful - like Dr. Martin Luther King (taught us to do) - if we have to!
( Susan's independently developed support DOC [ FOR " USA single-payer Health CARE" - still in progress. When ready, that PDF will be posted here [on my personal web site] ... ) till then> current researchNOTES
YES! You may use my hyperlinked notes, research, etc. & make your own document (or)... Please! - I urge everyone - only do USA "lawful" things.
"Never thinking a thing wrong - don't make it right." < Susan Marie CASSADY-Neuhart [ after Ms. Zora Neale Hurston ] < © 2017 - all rights reserved (by Susan)
Googled by Susan - 6-27-2017 : ( No results found for "Never thinking a thing wrong - don't make it right.". )
RESULT: https://www.google.com/search?q=%22Never+thinking+a+thing+wrong+-+don%27t+make+it+right.%22&rlz=1C1CHZL_enUS743US743&oq=%22Never+thinking+a+thing+wrong+-+don%27t+make+it+right.%22&aqs=chrome..69i57.2591j0j8&sourceid=chrome&ie=UTF-8
Also see: “A long habit of not thinking a thing wrong, gives it a superficial appearance of being right, and raises at first a formidable outcry in defense of custom.
But the tumult soon subsides. Time makes more converts than reason.” < Thomas Paine
Also, support your local politician Congress-person AND Senator - not by giving them ( these politicians ) your money; but, by reading the documents - the PNHP may have cited. Again, Susan provided the hyperlinks that follow. And, when the proposal's "Reference" was not clear - I provided more than one hyperlink.
[ GET INFORMED ! ] THEN, YOU CAN CREDIBLY "INFORM" AND TRY TO PERSUADE OTHERS... AND - VOTE!
1. Squires DA Explaining high health care spending in the United States: an international comparison of supply, utilization, prices, and quality. Commonwealth Fund Issue Brief. 2012;10:1‐14.
[ http://www.commonwealthfund.org/~/media/Files/Publications/Issue%20Brief/2012/May/1595_Squires_explaining_high_hlt_care_spending_intl_brief.pdf ]
2. Congressional Budget Office. Insurance Coverage Provisions of the Affordable Care Act—CBO’s March 2015 Baseline. Available at:
[ https://www.cbo.gov/sites/default/files/recurringdata/51298-2015-03-aca.pdf ] YES - THIS LINK WORKS!
3. Collins SR, Rasmussen PW, Beutel S, Doty MM. The Problem of Underinsurance and How Rising Deductibles Will Make It Worse—Findings from the Commonwealth Fund Biennial Health Insurance Survey. The Commonwealth Fund,. May 2015. ( MEDLINE Abstract Print ThisPrinter-FriendlyEmail This Email ThisDownload ThisDownload This)
[ http://www.bmj.com/content/350/bmj.h2786 ]
[ http://www.commonwealthfund.org/~/media/files/publications/issue-brief/2015/jan/1800_collins_biennial_survey_brief.pdf?la=en ]
[ https://www.milbank.org/quarterly/articles/one-nation-underinsured/ ]
4. Woolhandler S, Himmelstein DU. Life or Debt: Underinsurance in America. J Gen Intern Med. 2013;28(9):1122‐1124.
[ https://link.springer.com/article/10.1007/s11606-013-2460-y ]
[ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3744293/ ]
[ https://www.ncbi.nlm.nih.gov/pubmed/23615843# ]
5. Wharam JF, Zhang F, Landon BE, Soumerai SB, Ross‐ Degnan D. Low‐socioeconomic‐status enrollees in high‐ deductible plans reduced high‐severity emergency care. Health Aff (Millwood). 2013;32(8):1398‐1406.
[ http://content.healthaffairs.org/content/suppl/2013/07/25/32.8.1398.DC1/2012-1426_Wharam_Appendix.pdf ]
[ http://www.medscape.com/medline/abstract/23918484 ]
[ http://www.medscape.com/viewpublication/5894 ]
6. Galbraith AA, Soumerai SB, Ross‐Degnan D, Rosenthal MB, Gay C, Lieu TA. Delayed and forgone care for families with chronic conditions in high‐deductible health plans. J Gen Intern Med. 2012;27(9):1105‐1111.
[ https://www.ncbi.nlm.nih.gov/pubmed/22249829?access_num=22249829&link_type=MED ]
[ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3514993/ ]
7. Kullgren JT, Galbraith AA, Hinrichsen VL, et al. Health care use and decision making among lower‐income families in high‐deductible health plans. Arch Intern Med. 2010;170(21):1918‐1925.
[ http://jamanetwork.com/journals/jamainternalmedicine/fullarticle/226261 ]
[ YES - did downLoad PDF on 7-9-2017 ] On my computer: > JamaHealth*****CareUse112210_Refer7.pdf I plan to place this PDF on my "personal" web site.
8. Himmelstein DU, Thorne D, Warren E, Woolhandler S. Medical bankruptcy in the United States, 2007: results of a national study. Am J Med. 2009;122(8):741‐746.
[ http://www.amjmed.com/article/S0002-9343(09)00404-5/fulltext ]
[ http://www.amjmed.com/article/S0002-9343(09)00404-5/pdf ]
[ YES - did downLoad PDF on 7-9-2017 ] On my computer: _MedicalBK_resultsOFnationalStudy**** Reference8.pdf
9. Galbraith AA, Ross‐Degnan D, Soumerai SB, Rosenthal MB, Gay C, Lieu TA. Nearly half of families in high‐ deductible health plans whose members have chronic conditions face substantial financial burden. Health Aff (Millwood). 2011;30(2):322‐331.
[ http://www.childrenshospital.org/researchers/alison-galbraith ]
[ https://link.springer.com/article/10.1007/s11606-011-1970-8 ]
[ https://health.maryland.gov/mhqcc/Documents/meeting%20materials/High%20Deductible%20Health%20Plans%20Alison%20Galbraith%20MD%206-8-2012.pdf ]
[ https://connects.catalyst.harvard.edu/Profiles/profile/1245255/Network/CoAuthors/1237714 ] < does not work? "loading"
[ YES – this link does work >>>> https://connects.catalyst.harvard.edu/Profiles/display/Person/49840/Network/CoAuthors/Person/51129 ]
10. Woolhandler S, Himmelstein DU, Angell M, Young QD, Physicians' Working Group for Single‐Payer National Health I. Proposal of the Physicians' Working Group for Single‐Payer National Health Insurance. JAMA. 2003;290(6):798‐805.
[ http://www.atsjournals.org/doi/ref/10.1164/rccm.200906-0881ED ]
[ http://www.atsjournals.org/doi/pdf/10.1164/rccm.200906-0881ED ]
11. Himmelstein DU, Woolhandler S. A national health program for the United States. A physicians' proposal. N Engl J Med. 1989;320(2):102‐108 < - Got it ! See above
12. Comondore VR, Devereaux PJ, Zhou Q, et al. Quality of care in for‐profit and not‐for‐profit nursing homes: systematic review and meta‐analysis. BMJ.2009;339:b2732.
[ http://www.bmj.com/content/339/bmj.b2732 ]
13. Devereaux PJ, Heels‐Ansdell D, Lacchetti C, et al. Payments for care at private for‐profit and private not‐ for‐profit hospitals: a systematic review and meta‐ analysis. CMAJ. 2004;170(12):1817‐1824.
[ https://www.ncbi.nlm.nih.gov/pubmed/15184339 ]
[ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC419772/ ]
14. Silverman EM, Skinner JS, Fisher ES. The association between for‐profit hospital ownership and increased Medicare spending. N Engl J Med. 1999;341(6):420‐426.
[ http://www.dartmouthatlas.org/downloads/reports/Policy_Implications_Brief_022709.pdf ]
[ http://www.vaoutcomes.org/faculty/core/fisher/ ]
[ http://www.vaoutcomes.org/our_work/ ]
[ http://ajph.aphapublications.org/doi/full/10.2105/AJPH.91.9.1452 ]
[ http://www.harp.org/for-profit-nursing-homes-bad.htm ]
15. Sinnott SJ, Buckley C, O'Riordan D, Bradley C, Whelton H. The effect of copayments for prescriptions on adherence to prescription medicines in publicly insured populations; a systematic review and meta‐analysis. PLoS One. 2013;8(5):e64914.
[ http://researchonline.lshtm.ac.uk/2978931/1/journal.pone.0064914.PDF ]
[ http://researchonline.lshtm.ac.uk/2978931/ ]
16. Rasell ME. Cost sharing in health insurance‐‐a reexamination. N Engl J Med. 1995;332(17):1164‐1168.
[ http://www.nejm.org/doi/full/10.1056/NEJM199504273321711 ] <<<<<<<<< "the first 100 words appear "
17. Smolderen KG, Spertus JA, Nallamothu BK, et al. Health care insurance, financial concerns in accessing care, and delays to hospital presentation in acute myocardial infarction. JAMA.2010;303(14):1392‐1400.
[ http://jamanetwork.com/journals/jama/fullarticle/185673 ] <<< abstract
[ http://jamanetwork.com/journals/jama/fullarticle/185673#24846881 ]
[ https://www.saintlukeshealthsystem.org/doctor/paul-s-chan-md ]
[ https://www.ncbi.nlm.nih.gov/pubmed/20388895 ]
[ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3020978/ ]
18. Brook RH, Ware JE, Jr., Rogers WH, et al. Does free care improve adults' health? Results from a randomized controlled trial. N Engl J Med. 1983;309(23):1426‐1434.
[ https://www.ncbi.nlm.nih.gov/pubmed/6355851 ]
[ http://www.nejm.org/doi/full/10.1056/NEJM198312083092305 ]
19. Goldman DP, Joyce GF, Escarce JJ, et al. Pharmacy benefits and the use of drugs by the chronically ill. JAMA.2004;291(19):2344‐2350.
[ http://www.ihi.org/resources/Pages/Publications/Pharmacybenefitsandtheuseofdrugsbythechronicallyill.aspx ]
[ https://www.ncbi.nlm.nih.gov/pubmed/15150206?dopt=Abstract ]
[ http://jamanetwork.com/journals/jama/fullarticle/198761 ]
( REFERENCES CITED 20 - 46 ARE BEING WORKED ON NOW )
20. Welch HG, Sharp SM, Gottlieb DJ, Skinner JS, Wennberg JE. Geographic variation in diagnosis frequency and risk of death among Medicare beneficiaries. JAMA. 2011;305(11):1113‐1118.
[ https://www.ncbi.nlm.nih.gov/pubmed/?term=Geographic+variation+in+diagnosis+frequency+and+risk+of+death+among+Medicare+beneficiaries.+JAMA ]
21. Himmelstein DU, Jun M, Busse R, et al. A Comparison Of Hospital Administrative Costs In Eight Nations: US Costs Exceed All Others By Far. Health Aff (Millwood). 2014;33(9):1586‐1594.
[ https://bmchealthservres.biomedcentral.com/track/pdf/10.1186/s12913-014-0556-7?site=bmchealthservres.biomedcentral.com ]
PDF " Billing and insurance-related administrative costs in United States' health: synthesis of micro-costing evidence "
22. Schroeder SA, Frist W, National Commission on Physician Payment R. Phasing out fee‐for‐service payment. N Engl J Med. 2013;368(21):2029‐2032.
[ http://www.nejm.org/doi/full/10.1056/NEJMsb1302322 ]
23. Campbell JC, Ikegami N, Gibson MJ. Lessons from public long‐term care insurance in Germany and Japan. Health Aff (Millwood). 2010;29(1):87‐95.
[ https://www.ncbi.nlm.nih.gov/pubmed/20048365 ]
24. Frakt AB, Pizer SD, Feldman R. Should Medicare adopt the Veterans Health Administration formulary? Health Econ. 2012;21(5):485‐495.
[ https://experts.umn.edu/en/publications/should-medicare-adopt-the-veterans-health-administration-formular ]
25. Woolhandler S, Campbell T, Himmelstein DU. Costs of health care administration in the United States and Canada. N Engl J Med. 2003;349(8):768‐775.
[ https://www.ncbi.nlm.nih.gov/pubmed/12930930 ]
[ https://www.ncbi.nlm.nih.gov/pubmed/15088673 ]
26. Centers for Medicare & Medicaid Services. Table 19 National Health Expenditures by Type of Expenditure and Program.
https://www.cms.gov/research‐statistics‐data‐and‐systems/statistics‐trends‐and‐ reports/nationalhealthexpenddata/nationalhealthaccou ntshistorical.html [Accessed 10/06/15].
27. The Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. 2014
Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. Table II. B1. Available at:
http://www.cms.gov/Research‐ Statistics‐Data‐and‐Systems/Statistics‐Trends‐and‐ Reports/ReportsTrustFunds/downloads/tr2014.pdf [accessed March 19, 2015].
28. Woolhandler S, Himmelstein DU. Paying for national health insurance‐‐and not getting it. Health Aff (Millwood). 2002;21(4):88‐98. Woolhandler S, Himmelstein DU. "Paying for national health insurance‐‐and not getting it". Health Aff (Millwood). 2002;21(4):88‐98
[ http://www.jabfm.org/content/16/5/443.full ]
[ http://jamanetwork.com/journals/jama/article-abstract/182762 ] [ http://ajph.aphapublications.org/doi/pdf/10.2105/AJPH.2015.302997 ] PDF < ajph.2015.302997-Current ANDprojectedTAXpayer costs.pdf
29. Centers for Medicare and Medicaid Services. National Health Expenditure Projections 2012‐2022. Tables 2 and 2A. Available at
https://www.cms.gov/Research‐ Statistics‐Data‐and‐Systems/Statistics‐Trends‐and‐Reports/NationalHealthExpendData/Downloads/Proj20 12.pdf (accessed May 18, 2014).
30. Centers for Medicare & Medicaid Services. Accountable Care Organizations (ACO). Available at:
http://www.cms.gov/Medicare/Medicare‐Fee‐for‐ Service‐Payment/ACO/index.html?redirect=/aco (accessed January 27, 2014).
31. Ellwood PM, Jr., Anderson NN, Billings JE, Carlson RJ, Hoagberg EJ, McClure W. Health maintenance strategy. Med Care. 1971;9(3):291‐298.
32. Cooper AL, Kazis LE, Dore DD, Mor V, Trivedi AN. Underreporting high‐risk prescribing among Medicare Advantage plans: a cross‐sectional analysis. Ann Intern Med. 2013;159(7):456‐462.
33. Colla CH, Wennberg DE, Meara E, et al. Spending differences associated with the Medicare Physician Group Practice Demonstration. JAMA. 2012;308(10):1015‐1023.
34. Berenson RA. Shared Savings Program for accountable care organizations: a bridge to nowhere? Am J Manag Care. 2010;16(10):721‐726.
35. Song Z, Safran DG, Landon BE, et al. The 'Alternative Quality Contract,' based on a global budget, lowered medical spending and improved quality. Health Aff (Millwood). 2012;31(8):1885‐1894.
36. Curfman GD, Morrissey S, Drazen JM. High‐Value Health Care ‐‐ A Sustainable Proposition. N Engl J Med. 2013.
37. Lee TH. Putting the value framework to work. N Engl J Med. 2010;363(26):2481‐2483.
38. Porter ME. What is value in health care? N Engl J Med. 2010;363(26):2477‐2481.
39. Shahian DM, Wolf RE, Iezzoni LI, Kirle L, Normand SL. Variability in the measurement of hospital‐wide mortality rates. N Engl J Med. 2010;363(26):2530‐2539.
40. Hong CS, Atlas SJ, Chang Y, et al. Relationship between patient panel characteristics and primary care physician clinical performance rankings. JAMA. 2010;304(10):1107‐1113.
41. Lindenauer PK, Remus D, Roman S, et al. Public reporting and pay for performance in hospital quality improvement. N Engl J Med. 2007;356(5):486‐496.
42. Kristensen SW, Meacock R, Turner AJ, Boaden R, McDonald R, Roland M, Sutton M. Long‐Term Effect of Hospital Pay for Performance on Mortality in England. N Engl J Med 2014; 371:540‐548.
43. Jha AK, Joynt KE, Orav EJ, Epstein AM. The long‐term effect of premier pay for performance on patient outcomes. N Engl J Med. 2012;366(17):1606‐1615.
44. Eijkenaar F, Emmert M, Scheppach M, Schoffski O. Effects of pay for performance in health care: a systematic review of systematic reviews. Health Policy. 2013;110(2‐3):115‐130.
45. Committee on the Long‐Run Macroeconomic Effects of the Aging U.S. Population; Committee on Population‐‐ Phase II; Division of Behavioral and Social Sciences and Education; Board on Mathematical Sciences and Their Applications; Division on Engineering and Physical Sciences; The National Academies of Sciences, Engineering, and Medicine. The growing gap in life expectancy by income: Implications for federal programs and policy responses. Washington, DC: National Academies Press, 2015.
46. Committee on Public Health Strategies to Improve Health Board on Population Health and Public Health Practice. For the public’s health: Investing in a healthier future. Washington, DC: Institute of Medicine, 2012.
Susan's current research follows. Please feel FREE - to use my HYPERLINKED research - below (to make your own document).
hhh 
I can only hope you use this information - to HELP support HR676 - and, the good efforts of the DEMOCRATS & some REPUBLICANS
to finally make America a great country (again). Good LUCK! Please let me know - if I can HELP you. And, use the research - shown here - if you want to.
YES - thinking that it would be "helpful" (in April of 2017) - I did create a very early draft (of words) that I would like to see included in the final USA Health Care Bill.
( Susan's words PDF )
I am very open to discussing this "my early draft" proposal language - AND, my research (shown here) has caused my thinking to evolve greatly.
For example: Always design your User Interface system ( like the Venus Flytrap PLANT has done - through evolution)
------------------------- to ensure that you have caught a live bug worthy of consumption.
- Susan
- Please, send me a message If you want to) - by using my Contact form.
The Venus flytrap >  < " The Venus flytrap (also referred to as Venus's flytrap or Venus' flytrap), Dionaea muscipula, is a carnivorous plant native to subtropical wetlands on the East Coast of the United States in North Carolina and South Carolina. [A carnivorous plant] catches its prey—chiefly insects and arachnids—with a trapping structure formed by the terminal portion of each of the plant's leaves, which is triggered by tiny hairs on their inner surfaces. [FOR THIS SPECIES] 1) When an insect or spider crawling along the leaves contacts a hair, the trap prepares to close, snapping shut only 2) if another contact occurs within approximately twenty seconds of the first strike. The requirement of " redundant triggering " in this mechanism serves as a safeguard against wasting energy by trapping objects with no nutritional value, and 3) the plant will only begin digestion after five more stimuli to ensure it has caught a live bug worthy of consumption."
< " The Venus flytrap (also referred to as Venus's flytrap or Venus' flytrap), Dionaea muscipula, is a carnivorous plant native to subtropical wetlands on the East Coast of the United States in North Carolina and South Carolina. [A carnivorous plant] catches its prey—chiefly insects and arachnids—with a trapping structure formed by the terminal portion of each of the plant's leaves, which is triggered by tiny hairs on their inner surfaces. [FOR THIS SPECIES] 1) When an insect or spider crawling along the leaves contacts a hair, the trap prepares to close, snapping shut only 2) if another contact occurs within approximately twenty seconds of the first strike. The requirement of " redundant triggering " in this mechanism serves as a safeguard against wasting energy by trapping objects with no nutritional value, and 3) the plant will only begin digestion after five more stimuli to ensure it has caught a live bug worthy of consumption."
CAUTION READERS! Susan sent a message - containing 27 questions - to the "authors" of the 1989 document ( " A National Health Program for the United States: A Physicians' Proposal " ). At this page update, I have NOT heard back from them yet.
Albeit, it has only been hours since I sent them my message AND questions. ( link < Click for PDF display of the message & my questions. )
Now, to the "Venus flytrap" (above). As many of my readers are aware, I am educated in the biological sciences & experienced in creating software "User interfaces" [for USA military purposes, etc.] - and, documenting them. I am also (albeit poorly) educated in world 'history'. Thus, "those who cannot remember ... [ exactly what they learned at UWGB - circa 1979] are condemned to [fuzz the facts]" -apologies to George Santayana
As I first read the "Physicians' Proposal" 1989 document - referenced and copy provided above - I felt "they" - the Authors - seemed more concerned with HOW a "National Health Plan" would affect their peers ( other medical doctors ) - than average USA citizens - who would use the resulting system (as patients).
And, while on the one hand - this seemed natural - on the other hand, it seemed (to me) - a person [not a "medical doctor" - but, researching this issue greatly] - the very essence of the problem - THAT, of selling the "idea" for a National Health Program. That is - "who exactly" - is selling "what" to "whom". YES, I did get an 'A' in "Persuasion & Argumentation: Professor Clampitt. In fact, when building software User Interfaces AND writing software "User Manuals" - the very first task is always: Determing "exactly" who will use this technology "interface" or " User's document"?; That is, "Who is the intended audience ?" Thus, American Software Technical Writers [most often] aim their resulting documents at USA English speaking engineers - who may be only minimally familiar with math & physics; that is, as much as they are required to know - to accomplish their task. We make no assumptions. And, we fill in any anticipated holes of knowledge [ with examples and sidebars, etc.] - if, there is any doubt - the "End User" might not know enough... to use the product we are documenting. God forbid!The product results in embarrassing the "End-User".
Thus, I became slightly suspicious of the PNHP 1989 "poposal" - and, the PNHP web site. Consider, in the USA - there are nearly ONE Million licensed Medical Doctors (A) - serving 47 different specialties (B) - but, the "membership" of this " PNHP organization" is only (they say- 2017) 20,000 licensed medical doctors. (C) Thus, the PNHP represents (by their posted numbers) only about 2% of the total number of USA medical doctors. So, why did they (the authors) create this document - at all? [in 1989] Are they trying to sell - an idea? If yes. To whom? My read - of their document - made it clear (to me) - that USA medical doctors - and USA medical insurance selling entities - will be big financial losers - in their "proposed USA national health plan". Doctors would have 3 options for remuneration - for their services. Given the requirements to become a USA medical doctor (D) - this (alone) - must be horrifying - for the 'other' 98% of USA medical doctors - who are not members - of the PNHP. Again, why did they (the authors) create this document - at all? [in 1989] Then, I thought of the Venus Flytrap - and, how some organisms use a strategy of "attraction" - only to identify and capture those they intend to eat. Then again - sometimes those organisms that arrive - are the Venus Flytrap's undoing. That is, 1) they are poisonous - or 2) there is so little return in consuming them - the Venus Flytrap dies. I hope the Authors - of the PNHP 1989 document ( " A National Health Program for the United States: A Physicians' Proposal " ).) will answer my 27 posed questions. I will share them (here on my personal web site) - if they give me permission to do so. Also, if their replies allay my concerns - that those who join them are being captured - only to be eaten - I will state so.
In America, we are encouraged to "hand-off" responsibility - as the circumstances seem appropriate, proper and permit. (For example, a wallet or purse - containing credit cards, money, etc.- found laying on a chair. "Americans" - upon finding this object - will instantly - retrieve - then, look-for the "Lost and Found" department. Thus, relieving themselves of further responsibility. ) I only caution my readers, do NOT "hand-off" YOUR responsibility for a Single-Payer Health Plan - to others - like the PNHP Organization - particularly - if they represent only 2% of USA Medical Doctors, the AMA AND the USA Insurance Companies [they - (the doctors) - may be in league with]. YOU! - the consumer of medical services - must VOTE - for a National Health Plan - that serves YOU! GET INFORMED & VOTE !
For example, the AMA document "AMA VISION ON HEALTH REFORM "- that I just "downloaded" is a sham - that ONLY (really) supports USA 'Health Insurance' companies .
THE AMA IS OUR ENEMY!
"You have enemies? Good. That means you've stood up for something sometime in your life." Winston Churchill ~ Original sentiment by the French author - Victor Hugo in Villemain (1845), as follows: " You have enemies? Why, it is the story of every man who has done a great deed or created a new idea. It is the cloud which thunders around everything that shines. Fame must have enemies, as light must have gnats. Do not bother yourself about it; disdain. Keep your mind serene as you keep your life clear. ( https://archiveshub.jisc.ac.uk/search/archives/94848e4b-55bd-3cef-b9ee-893e77082509?component=6ea1f6f0-a2d8-37f3-abef-878caa81acb6 )
A proposal FOR Health Care for ALL Americans [ as Proposed in 1989 - PDF ]
< "A National Health Program for the United States: A Physicians' Proposal"
Links to the original document - on the in-situ web site:
http://www.pnhp.org/publications/a_national_health_program_for_the_united_states.php?page=all
A Proposal made in - 1989 http://www.pnhp.org/sitemap/ < other proposals are also posted here
< Susan is reading and sprucing this 1989 document up NOW. ] I will do my very best - NOT to "take credit" - for what other Americans - did come up with - in 1989.
( Susan's independently developed support DOC - still in progress - that PDF will be posted here ... ) current researchNOTES YES, you may use my hyperlinked notes, research & make your own document (or)...
PDF ( WORK on 7-4-2017 ) < Susan's in-progress "clarification" and UP-date to the 1989 Original proposal - Susan has many questions for the Authors of the document.
Susan sent a message - containing 27 questions ( link ) ( - to the "authors" of the 1989 document ( " A National Health Program for the United States: A Physicians' Proposal " ).
At this page update, I have NOT heard back from them yet.
Albeit, it has only been hours since I sent them my message AND questions. ( link < Click for PDF display of the message & my questions. )
An "outline" of the Original ( 1989 ) proposal: [ this "outline" is included - in a vertical format - in the "edited PDF above ]
COVERAGE, PAYMENT FOR HOSPITAL SERVICES, PAYMENT FOR PHYSICIANS' SERVICES, AMBULATORY CARE, AND MEDICAL HOME CARE
( Fee-for-Service Payment - Global Budgets - Capitation ) PAYMENT FOR LONG-TERM CARE, ALLOCATION OF CAPITAL FUNDS, HEALTH PLANNING, AND RETURN ON EQUITY
PUBLIC, ENVIRONMENTAL, AND OCCUPATIONAL HEALTH SERVICES PRESCRIPTION DRUGS AND SUPPLIES
FUNDING: Medicare and Medicaid - Employer Contributions - Private Insurance Revenues - General Tax Revenues
DISCUSSION: The Patient's View - The Practitioner's View - The Effect on Other Health Workers - The Effect on Hospitals - The Effect on the Insurance Industry - The Effect on Corporate America - Health Benefits and Financial Costs - Unsolved Problems - Political Prospects
REFERENCES
Why do we need Health Insurance companies - at all? < Google this question - The following is just "some" of what you get.
https://www.counterpunch.org/2009/03/26/why-do-we-need-a-health-insurance-industry/
http://health.usnews.com/health-care/health-insurance/articles/2016-11-01/why-do-you-need-health-insurance
http://www.kevinmd.com/blog/2012/03/america-health-insurance-companies.html
https://www.quora.com/Why-do-we-need-health-insurance-companies
https://www.forbes.com/sites/michaelbell/2013/02/19/why-spend-900-billion-on-health-insurance/#1949ca7d27bf
http://articles.latimes.com/2010/feb/28/business/la-fi-hiltzik28-2010feb28
http://thehill.com/blogs/pundits-blog/healthcare/302965-to-fix-healthcare-lets-get-rid-of-insurance-companies
http://fortune.com/2014/10/20/health-insurance-future/
Are Health Insurance companies "parasites" ? "Parasitism" is one form of symbiosis. There are three others.
What form of "relationship" do doctors form with their patients ? https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1496871/
1) A parasite benefits at the expense of the host. (parasitism)
2) Commensalism, in biology, is a relationship between individuals of two species in which one species obtains food or other benefits from the other without either harming or benefiting the latter. https://en.wikipedia.org/wiki/Commensalism
3) This is in contrast with mutualism, in which both organisms benefit from each other.
4) Amensalism, is an association between organisms of two different species in which one is inhibited or destroyed and the other is unaffected. There are two basic modes:
a) competition, in which a larger or stronger organism excludes a smaller or weaker one from living space or deprives it of food,
and b) antibiosis, in which one organism is unaffected but the other is damaged or killed by a chemical secretion.
https://www.merriam-webster.com/dictionary/symbiosis
https://www.cdc.gov/parasites/about.html
https://en.wikipedia.org/wiki/Symbiosis
All fungi are heterotrophs ( https://en.wikipedia.org/wiki/Heterotroph ). Fungi are either parasites or saprobes. Fungi have parasitic hyphae = for example, haustoria https://en.wikipedia.org/wiki/Haustorium
A host–parasite system: Some medical doctors participate in "host–parasite" systems.
health insurance rescission < Google Medical insurance practice on trial < Google
If medical insurance [the practice] is a "parasite" - should USA law be created - which makes it illegal to sell "medical insurance" to a "host" society - of Americans?
http://www.washingtonpost.com/wp-dyn/content/article/2009/09/07/AR2009090702455.html "... Rescission -- the technical term for canceling coverage on grounds that the company was misled -- is often considered among the most offensive practices in an insurance industry that already suffers from a distinct lack of popularity among the American public. Tales of cancellations have fueled outrage among regulators, analysts, doctors and, not least, plaintiffs' lawyers, who describe insurers as too eager to shed patients to widen profits."
Bacteria and their conjugative plasmids can also provide a tractable model of a host–parasite system. > http://www.nature.com/ismej/journal/v3/n7/full/ismej200922a.html < "... (last paragraph of report) This work also has implications outside of plasmid biology, in which our mathematical model could apply to any host–parasite system that fits its basic assumptions. In general terms, we predict that a parasite may be selected for in the environment if it provides protection from a more virulent pathogen. The competitive advantage we observed for a low-cost (that is, low-virulence) parasitic element provides a valuable contrast to studies that predict or demonstrate an increase in virulence under competitive pressure for other parasites (Kover et al., 1997; Kover and Clay, 1998; Kerr et al., 2006; Coombs et al., 2007; Bull and Ebert, 2008). We postulate that the importance of vertical transmission and the resistance of the infected host to superinfection are key factors that support a competitive reduction in virulence in our system. Theoretical work suggests that frequent vertical inheritance under competitive conditions might limit virulence in other parasites as well (Frank, 1996). Understanding factors that drive evolution of virulence or temperance will provide insights into the spread of infectious diseases and allow us to better determine which infectious agents require particular attention as new pathogens emerge. ...
https://en.wikipedia.org/wiki/Host%E2%80%93parasite_coevolution
https://en.wikipedia.org/wiki/Bacterial_conjugation
a beneficial parasite
http://citybugs.tamu.edu/2013/08/02/what-is-a-beneficial-parasite/
"... The words “beneficial” and “parasite” are not normally heard together. But when talking about gardens, and parasitic wasps that attack pests, the word pairing makes good sense.
Many insects in both natural settings and the urban landscape have long been recognized by humans as “beneficial”, as in benefiting man. Predators of pest insects, in particular, have attracted admiring fans, especially farmers. As early as ninth century China, farmers were modifying their orchards to aid the transfer of predator ants for control of citrus pests. By the 18th century birds, ground beetles and lady beetles were recognized as important controllers of pests. Today when someone mentions good bugs, most gardeners quickly point to dragonflies, green lacewings, preying mantids and lady beetles as brave defenders of the garden.
But in addition to these relatively large and showy predators, a whole class of helpful garden insects often are unnoticed, unappreciated, and (sometimes) abused. They are the beneficial parasites, or more correctly, “parasitoids” of the garden. In nature parasites usually only weaken or sicken their hosts. Parasitoids kill and actually consume their prey. Unlike predators which are highly mobile and consume multiple prey, parasitoids are not very mobile (in the immature stages) and typically feed on only one host. The first known parasitoid wasps, called “ichneumons”, were discovered laying eggs on caterpillars and described by anatomists and microscopists in the early 1700s. After the ichneumon larvae hatched, they penetrated and fed on their hosts in a gruesome internal attack. By killing their hosts in this way, ichneumons were found to provide an excellent way to control pests.
We can thank benefical parasites that our gardens are not constantly overrun with pests like these aphids.
Today we recognize hundreds of wasps, flies and (a few) beetles as insect parasitoids. Besides the ichneumon wasps, dozens of other wasp and fly parasitoid families have been discovered. We now know that parasitoid insects tend to be very closely attuned to their hosts, and are often specialized on only one or a few closely related species of prey. Thanks to specialization, parasitoids are usually very adept at finding pests before the pests become abundant. The fact that insect pests rarely take over gardens or landscapes is due, in large part, to the presence of parasitoids working quietly behind the scenes.
As more of the natural landscape is urbanized, gardeners face a challenge. How do we maintain the right environment to preserve and protect the natural hide-and-seek relationship between parasitoids and predators and their prey? If we ignore the needs of beneficial insects, we can expect pest problems to become more frequent and more severe.
It turns out that parasitoids can do well in urban landscapes and gardens when provided with food and shelter in the form of a diverse landscape–especially landscapes with native plants. In addition, parasitoids must be protected from toxic insecticides.
Because of their relatively small size, parasitoids are extremely sensitive to some insecticides. Here are three ways you can use pesticides while preserving beneficial parasites:
- 1) Spray selectively. Most insect pest attack only one or a few types of closely related plants. By spraying only the types of plants under attack, you solve your pest problem and give parasitoids other plants to feed and hide on, free from insecticide residues.
- 2) Use low impact pesticides. Some insecticides are inherently safer for small natural enemies, either because they break down quickly after spraying or because they are highly selective for the target pest. For examples of low impact pesticides, click here.
- 3) Avoid spraying plants, especially those in flower, during the day. Most beneficial insects are active during the day. By spraying at dusk or at night you can avoid spraying beneficials directly.
Parasitic wasps are among the most effective and common parasitoids in the garden, yet few gardeners notice them. These tiny insects lay their eggs either inside or on their host. Once these eggs hatch, the wasp larvae develop on the internal blood and tissues of the host, eventually killing it. Although one parasitoid only kills one host, each female parasitoid lays her eggs in dozens or hundreds of hosts. Some parasitoid wasps only attack one species of pest, so using these insects in biological control programs can be difficult due to the need to choose the right species of parasitoid and know exactly what pest is present. The empty shell of the host left behind after a parasitoid attack is often called a “mummy”.
http://www.encyclopedia.com/science/encyclopedias-almanacs-transcripts-and-maps/episomes-plasmids-insertion-sequences-and-transposons
Episomes, plasmids, insertion sequences, and transposons are elements of DNA (deoxyribonucleic acid ) that can exist independent of the main, or genomic, DNA.
An episome is a non-essential genetic element. In addition to its independent existence, an episome can also exist as an integrated part of the host genome of bacteria . It originates outside the host, in a virus or another bacterium. When integrated, a new copy of the episome will be made as the host chromosome undergoes replication. As an autonomous unit, the viral episome genetic material destroys the host cell as it utilizes the cellular replication machinery to make new copies of itself. But, when integrated into the bacterial chromosome they multiply in cell division and are transferred to the daughter cells. Another type of episome is called the F factor. The F factor is the best studied of the incompatibility groups that have the property of conjugation (the transfer of genetic material from one bacterial cell to another). The F factor can exist in three states. 1) F+ is the autonomous, extrachromosomal state. 2) Hfr (or high frequency recombination ) refers to a factor, which has integrated into the host chromosome. 3) Finally, F, or F prime, state refers to the factor when it exists outside the chromosome, but with a section of chromosomal DNA attached to it. An episome is distinguished from other pieces of extrachromosomal DNA, such as plasmids, on the basis of their size. Episomes are large, having a molecular weight of at least 62 kilobases.
In contrast to episomes, a plasmid exists only as an independent piece of DNA. It is not capable of integration with the chromosomal DNA; it carries all the information necessary for its own replication. In order to maintain itself, a plasmid must divide at the same rate as the host bacterium. A plasmid is typically smaller than an episome, and exists as a closed circular piece of double stranded DNA. A plasmid can be readily distinguished from the chromosomal DNA by the techniques of gel electrophoresis or cesium chloride buoyant density gradient centrifugation. In addition to the information necessary for their replication, a plasmid can carry virtually any other gene . While not necessary for bacterial survival, plasmids can convey a selective advantage on the host bacterium. For example, some plasmids carry genes encoding resistance to certain antibiotics . Such plasmids are termed resistance or R factors. Other traits carried on plasmids include degradation of complex macromolecules, production of bacteriocins (molecules that inhibit bacterial growth or kill the bacteria), resistance to various heavy metals, or diseasecausing factors necessary for infection of animal or plant hosts. Such traits can then be passed on to other bacteria, as some (but not all) plasmids also have the ability to promote transfer of their genetic material, in a process called conjugation. Conjugation is a one-way event—the DNA is transferred from one bacterium (the donor) to another bacterium (the recipient). All plasmids belong to one of the 30 or more incompatibility groups. The groups determine which plasmids can co-exist in a bacterial cell and help ensure that the optimum number of copies of each plasmid is maintained. Plasmids have been exploited in molecular biology research. The incorporation of genes into plasmids, which maintain large numbers of copies in a cell (so-called multicopy plasmids), allows higher levels of the gene product to be expressed. Such plasmids are also a good source of DNA for cloning .
Transposons and insertion sequences are known as "mobile genetic elements". While they can also exist outside of the chromosome, they prefer and are designed to integrate into the chromosome following their movement from one cell to another. The are of interest to researchers for the insight they provide into basic molecular biology and evolution , as well as for their use as basic genetic tools. Transposons contain genes unrelated to the transposition of the genetic material from one cell to another. For example, Class 1 transposons encode drug resistance genes. In contrast, insertion sequences encode only the functions involved in their insertion into chromosomal DNA. Both transposons and insertion sequences can induce changes in chromosomal DNA upon their exiting and insertions, and so can generate mutations .
“Medicine is a science of uncertainty and an art of probability”. —William Osler ( https://en.wikipedia.org/wiki/William_Osler )
This statement sums up the life of a doctor quite nicely. Of course, there is no such thing as a “typical” day. Each day is different, and there are many types of doctors.
There are gynaecologists, endocrinologists, oncologists, gastroenterologists and the list is endless. [ no it is not an "endless list ] https://www.bioexplorer.net/types-of-doctors/
S, it is very natural that their life can’t be the same. So, here is a description of how a day of a doctor really looks like.
A Typical Day in the Life of a Doctor
Well, the eight or more hours of work are all about back-to-back meetings. A doctor’s bread and butter is seeing patients, and each appointment is essentially a meeting with a client. You check the details of the case, try and get a sense of what’s going on, and then figure out the medicines–often trying to do this within a half hour.
The thinking process is a lot like troubleshooting a broken device, only it’s from a foreign manufacturer. You possess thousands of different but crude tools, and you can only try to fix the device so many times. When someone comes in with a complaint, you think of a bunch of things it could be (your differential diagnosis) and then ask questions to try and narrow it down and separate it from similar problems. Then you choose your tests and hope that you can pin down the source of the problem to something in particular (your diagnosis). Then you figure out if the problem is fixable.
The finer details of the job depend on the work setting. If you work in a hospital on a medical team, it’s like being an officer in the military, or a middle manager in a large company. Middle managers don’t do the grunt work–you’re paid to figure out what work needs to be done, make sure that the work is done, and bear the responsibility of right and wrong decisions. It is accomplished by a lot of paperwork–meeting patients to find out their issues, documenting your findings and your thinking process, writing orders, communicating those orders to other healthcare professionals to act on them.
If you work in a clinic, it’s more like being a small business owner. The work is the same, but you have a bit more autonomy and control over the setup, though you aren’t able to get your results or make changes quite as quickly. We spoke to some doctors to understand what their routine is to better understand the point in question.
Dr. Sheryl D’souza
“I work four days a week for about 10 hours a day. I have my own clinic as well as work for a well-known hospital. My day usually starts at 9 am, and I prefer taking new patients first as they take more time than follow-ups. Since I am a neurologist, I have to sometimes rush for emergency cases to the hospital and take care of the patients. I spend a considerable time in reading up the patient history before I start my day. After having back-to-back patients till 1 pm, I come home for quick lunch. I go the hospital in the evening, and it’s the same routine of seeing patients.
I am also involved with my children’s schools and sports activities, so I make it a point that I squeeze in some time for it. I enjoy my work but I work hard, and then in late evenings, I spend time with my family and friends.
I also travel for meetings and conferences. I usually take my family with me on these trips so they can enjoy the experience of new cities.
Dr. Akshita Shetty
“I don’t have a typical day. I generally begin the day performing rounds at the hospital. This involves going to various patients (such as the newborn nursery and paediatric ward), where he/she visits with the patient’s family members, takes vitals and checks the patient’s status. After two or three hours of rounds, I go to my private office to begin patient appointments. The busyness of the day sometimes depends on the season – for example, wintertime tends to be a busier season for paediatric appointments due to flu season and other wintertime ailments. Throughout afternoon, I am generally signing forms, writing prescriptions and conducting other necessary paperwork. Most of the times, I end my day around 6:30 or 7:00 p.m., but this varies.
Overall, my day is very busy. Patient appointments are one small part of a paediatrician’s job – but that small part impacts the lives of many people. I try not to schedule anything work-related on the weekends, but we occasionally have community outreach events that take some time.
This is how it’s like to be a practising doctor. It’s hard to describe one day because every day is very different. As long as doctors come equipped with a great attitude and a stethoscope, their is exciting with many opportunities to learn and develop their clinical skills.
HHHHHHHHHHHHHHHHHHHHHHHHHHHHHHHHHHHHH
Hhhhh TYPES of medical doctors hhhh 47 of them hhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhh
https://www.bioexplorer.net/types-of-doctors/
Types of Doctors: In a nutshell, medical professionals, or simply doctors, help in the diagnosis, management, and treatment of various diseases. Hence, if you have ever become so ill that you had to visit a doctor, you know exactly how important their job is.
- Types of Doctors (Medical)
- Other Types of Doctors / Health Professionals (Non-Medical)
When dealing with a specific health illness, it is important to provide the best possible medication and treatment. To do that, one needs to determine which type of medical professional is suited to treat that condition. But the medical field, like in any other fields in the industry, is made up of different types of doctors and specialists. Their intense and rigorous medical training have demanded them not only to master at least the basics of scientific discipline which include anatomy, cell biology, physiology, epidemiology, pharmacology, nutrition, and so on but also to specialize in their chosen specific field. In order to give an overview, below is a list of the complete & comprehensive 56 different types of doctors & health care professionals (both medical and non-medical) and the area they specialize in.
Types of Doctors (Medical)
#1 Allergist
#2 Anaesthesiologist / Anasthesiologist / Anesthesiologist
#3 Andrologist
#4 Cardiologist
#5 Cardiac Electrophysiologist
#6 Dermatologist
#7 Emergency Medicine / Emergency (ER) Doctors
#8 Endocrinologist
#9 Epidemiologist
#10 Family Medicine Physician
#11 Gastroenterologist
#12 Geriatrician
#13 Hyperbaric Physician
#14 Hematologist
#15 Hepatologist
#16 Immunologist
#17 Intensivist
#18 Internal Medicine Specialist
#19 Maxillofacial Surgeon / Oral Surgeon
#20 Medical Geneticist
#21 Neonatologist
#22 Nephrologist
#23 Neurologist
#24 Neurosurgeon
#25 Nuclear Medicine Specialist
#26 Obstetrician/Gynecologist (OB/GYN)
#27 Oncologist
#28 Ophthalmologist
#29 Orthopedic Surgeon / Orthopedist
#30 Otolaryngologist (also ENT Specialist)
#31 Parasitologist
#32 Pathologist
#33 Perinatologist
#34 Periodontist
#35 Pediatrician
#36 Plastic Surgeon
#37 Psychiatrist
#38 Pulmonologist
#39 Radiologist
#40 Rheumatologist
#41 Sleep Doctor / Sleep Disorders Specialist
#42 Spinal Cord Injury Specialist
#43 Sports Medicine Specialist
#44 Surgeon
#45 Thoracic Surgeon
#46 Urologist
#47 Vascular Surgeon
#48 Veterinarian :: veterinarians are responsible for the treatment of sick animals.
Allied Health Professionals
#1 Audiologist
#2 Chiropractor
#3 Diagnostician
#4 Microbiologist
#5 Palliative care specialist
#6 Pharmacist
#7 Physiotherapist
#8 Podiatrist / Chiropodist
[ end of copy 6-30-2017 ]
<<<<<< This needs to be changed to "Single Payer Health CARE" >>>>
https://en.wikipedia.org/wiki/Universal_health_care
Universal health care, sometimes referred to as universal health coverage, universal coverage, or universal care, usually refers to a health care system that provides health care and financial protection to all citizens of a particular country. It is organized around providing a specified package of benefits to all members of a society with the end goal of providing financial risk protection, improved access to health services, and improved health outcomes.[2] Universal health care is not one-size-fits-all and does not imply coverage for all people for everything. Universal health care can be determined by three critical dimensions: who is covered, what services are covered, and how much of the cost is covered.[2] It is described by the World Health Organization as a situation where citizens can access health services without incurring financial hardship.[3] U.N. member states have agreed to work toward universal health coverage by 2030.[4]
https://en.wikipedia.org/wiki/Single-payer_healthcare
Single-payer healthcare is a healthcare system in which the state, financed by taxes, covers basic healthcare costs for all residents regardless of income, occupation, or health status. The alternatives include "multi-payer" systems in which private individuals or their employers buy health insurance or healthcare services from private or public providers.[1][2][3]
Single-payer systems may contract for healthcare services from private organizations (as is the case in Canada) or may own and employ healthcare resources and personnel (as is the case in the United Kingdom). "Single-payer" describes the mechanism by which healthcare is paid for by a single public authority, not the type of delivery or for whom physicians work. In contrast, multi-payer healthcare uses a mixed public-private system.
" Securing Universal Health Care : Democrats believe that health care is a right, not a privilege, and our health care system should put people before profits. Thanks to the hard work of President Obama and Democrats in Congress, we took a critically important step toward the goal of universal health care by passing the Affordable Care Act, which has covered 20 million more Americans and ensured millions more will never be denied coverage because of a pre-existing condition. Democrats will never falter in our generations-long fight to guarantee health care as a fundamental right for every American. As part of that guarantee, Americans should be able to access public coverage through a public option, and those over 55 should be able to opt in to Medicare. Democrats will fight any attempts by Republicans in Congress to privatize, voucherize, or “phase out” Medicare as we know it. We will keep fighting until the ACA’s Medicaid expansion has been adopted in every state. Nineteen states have not yet expanded Medicaid. This means that millions of low-income Americans still lack health insurance and are not getting the care they need. Additionally, health care providers, clinics, hospitals, and taxpayers are footing a higher bill when people without insurance visit expensive emergency rooms.
Supporting Community Health Centers: We must renew and expand our commitment to Community Health Centers, as well as community mental health centers and family planning centers. These health centers provide critically important, community-based prevention and treatment in under -served communities, prevent unnecessary and expensive trips to emergency rooms, and are essential to the successful implementation of the ACA. We will fight for a comprehensive system of primary health care, including dental, mental health care, and low-cost prescription drugs by doubling of funding for federally qualified community health centers over the next decade, which currently serve 25 million people. Democrats also know that one of the key ingredients to the success of these health centers is a well-supported and qualified workforce in community-based settings. We will fight to train and support this workforce, encourage providers to work with under served populations through the National Health Service Corps, and create a comprehensive strategy to increase the pool of primary health care professionals. Democrats are committed to investing in the research, development, and innovation that creates lifesaving drugs and lowers overall health costs, but the profiteering of pharmaceutical companies is simply unacceptable. " [ It is important to know this. However, Susan should not be "preachin' to the choir". ] https://www.democrats.org
https://www.democrats.org/party-platform
https://www.congress.gov/bill/115th-congress/house-bill/676 Summary: H.R.676 — 115th Congress (2017-2018)All Information (Except Text)
There is one summary for H.R.676. Bill summaries are authored by CRS. Shown Here: Introduced in House (01/24/2017)
Expanded & Improved Medicare for All Act [ bill summary ]
This bill establishes the Medicare for All Program to provide all individuals residing in the United States and U.S. territories with free health care that includes all medically necessary care, such as primary care and prevention, dietary and nutritional therapies, prescription drugs, emergency care, long-term care, mental health services, dental services, and vision care.
Only public or nonprofit institutions may participate. Nonprofit health maintenance organizations (HMOs) that deliver care in their own facilities may participate.
Patients may choose from participating physicians and institutions.
Health insurers may not sell health insurance that duplicates the benefits provided under this bill. Insurers may sell benefits that are not medically necessary, such as cosmetic surgery benefits.
The bill sets forth methods to pay institutional providers and health professionals for services. Financial incentives between HMOs and physicians based on utilization are prohibited.
The program is funded: (1) from existing sources of government revenues for health care, (2) by increasing personal income taxes on the top 5% of income earners, (3) by instituting a progressive excise tax on payroll and self-employment income, (4) by instituting a tax on unearned income, and (5) by instituting a tax on stock and bond transactions. Amounts that would have been appropriated for federal public health care programs, including Medicare, Medicaid, and the Children's Health Insurance Program (CHIP), are transferred and appropriated to carry out this bill.
The program must give employment transition benefits and first priority in retraining and job placement to individuals whose jobs are eliminated due to reduced clerical and administrative work under this bill.
The Department of Health and Human Services must create a confidential electronic patient record system.
The bill establishes a National Board of Universal Quality and Access to provide advice on quality, access, and affordability.
The Indian Health Service must be integrated into the program after five years. Congress must evaluate the continued independence of Department of Veterans Affairs health programs.
( 6 – 28 – 2017) Dear OhiO Senator Brown,
I hope my message finds you well. As you may recall (Sir), I am the Dayton, Ohio lady - that is creating a “personal” web site. [ https://hansandcassady.org/ ] I am in support of Health Care (for all Americans ) – that is “paid for” in a manner - similar to the way that Social Security funds are collected from all Americans (via payroll taxes) – and then provided (as services) – to Americans - when needed. It has come to my attention – that what I want to see enacted – is most properly called “ Single-payer healthcare” [ see citation below ]. BUT, the Democratic Party National Platform [ see citation below] – uses the terminology “ Universal health care” [ circa page 31] (https://www.democrats.org/party-platform).
Thus, for me to be in “perfect accord” with the DNC platform – I hope that terminology is soon changed – or, at least clarified. Sir, I support the sentiments expressed by Congressman John Conyer’s bill [HR 676] – however, his bill does not include the idea – so far – only publicly expressed by me. ( A retired lady - that is not elected to any public office. Nor, do I care to be.)
Sir, because, I do not see the benefit of Medical Insurance services ( at all) at this point – as the concept – of “insurance” - was originally brought forth by the Greeks [“communal interest” and “risk sharing”] -and, as this concept (of insurance) is applied to Medical services (for all Americans) – and, the end of needless pain & suffering [ today]. Sir, as a professional writer (before my stroke) I am (albeit) slowly preparing a document – which I will post to my personal web site - that (I hope) helps answer the question: “Why do we need Health Insurance companies - at all?
Sir, after finishing my research and creating the document [ supporting any resulting thesis] I hope you will be willing to support legislation (from the US House) - regarding a USA law be made – that it is illegal to sell “Health Insurance” in America.
As you may be aware, the AMA – vigorously opposed President Truman & FDR (long ago) – when they had the same ideas. Thus, the Medical Industry – as represented by the AMA (today) – will probably be against any research (like mine) – and, any proposed legislation that results – from my efforts. Thus, I propose we prepare ( now!) for their objections. I will share my thoughts with OhiO Senator Portman - and, other Ohio politicians (as well).
I hope that you and Senator Portman can continue to work together on the Health Care issue. I appreciate that he – and other REPUBLICAN politicians have been brave – recently – to oppose their party leader ( Mr. Trump). I did request him to do this. OhiO Congressman Mike Turner [OH10] also did this - oppose Mr. Trump.
And, please be aware – that because (of my business experience & background) I recognize that Mr. Trump thinks – first & foremost – like a “businessman”. Thus, even he may be willing to go along – with the notion of “getting rid of medical insurance companies altogether”. Nobody likes a parasite – and, Mr. Trump – because he thinks like a “businessman” – probably hates the idea of a “parasite” on the USA Health Care system; which, from my research (thus far) – that is exactly what the Medical Insurance industry is today.
Sir, we may also need Tort reform laws – related to the USA Medical Care industry.
https://en.wikipedia.org/wiki/Universal_health_care
Universal health care, sometimes referred to as universal health coverage, universal coverage, or universal care, usually refers to a health care system that provides health care and financial protection to all citizens of a particular country. It is organized around providing a specified package of benefits to all members of a society with the end goal of providing financial risk protection, improved access to health services, and improved health outcomes.[2] Universal health care is not one-size-fits-all and does not imply coverage for all people for everything. Universal health care can be determined by three critical dimensions: who is covered, what services are covered, and how much of the cost is covered.[2] It is described by the World Health Organization as a situation where citizens can access health services without incurring financial hardship.[3] U.N. member states have agreed to work toward universal health coverage by 2030.[4]
https://en.wikipedia.org/wiki/Single-payer_healthcare
Single-payer healthcare is a healthcare system in which the state, financed by taxes, covers basic healthcare costs for all residents regardless of income, occupation, or health status. The alternatives include "multi-payer" systems in which private individuals or their employers buy health insurance or healthcare services from private or public providers.[1][2][3]
Single-payer systems may contract for healthcare services from private organizations (as is the case in Canada) or may own and employ healthcare resources and personnel (as is the case in the United Kingdom). "Single-payer" describes the mechanism by which healthcare is paid for by a single public authority, not the type of delivery or for whom physicians work. In contrast, multi-payer healthcare uses a mixed public-private system.z
https://www.democrats.org/party-platform
“ Securing Universal Health Care : Democrats believe that health care is a right, not a privilege, and our health care system should put people before profits.”
https://www.congress.gov/bill/115th-congress/house-bill/676
https://hansandcassady.org/
hhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhh 937-985-9399
( 6 – 28 – 2017) Dear OhiO Senator Portman
I hope my message finds you well. As you may recall (Sir), I am the Dayton, Ohio lady - that is creating a “personal” web site. [ https://hansandcassady.org/ ] I am in support of Health Care (for all Americans ) – that is “paid for” in a manner - similar to the way that Social Security funds are collected from all Americans (via payroll taxes) – and then provided (as services) – to Americans - when needed.
I am a registered DEMOCRAT.
It has come to my attention – that what I want to see enacted – is most properly called “ Single-payer healthcare” [ see citation below ]. BUT, the Democratic Party National Platform [ see citation below] – uses the terminology “ Universal health care” [ circa page 31] (https://www.democrats.org/party-platform).
Thus, for me to be in “perfect accord” with the DNC platform – I hope that terminology is soon changed – or, at least clarified. Sir, I support the sentiments expressed by Congressman John Conyer’s bill [HR 676] – however, his bill does not include the idea – so far – only publicly expressed by me. ( A retired lady - that is not elected to any public office. Nor, do I care to be.)
Sir, because, I do not see the benefit of Medical Insurance services ( at all) at this point – as the concept – of “insurance” - was originally brought forth by the Greeks [“communal interest” and “risk sharing”] -and, as this concept (of insurance) is applied to Medical services (for all Americans) – and, the end of needless pain & suffering [ today]. Sir, as a professional writer (before my stroke) I am (albeit) slowly preparing a document – which I will post to my personal web site - that (I hope) helps answer the question: “Why do we need Health Insurance companies - at all?
Sir, after finishing my research and creating the document [ supporting any resulting thesis] I hope you will be willing to support legislation (from the US House) - regarding a USA law be made – that it is illegal to sell “Health Insurance” in America.
As you may be aware, the AMA – vigorously opposed President Truman & FDR (long ago) – when they had the same ideas. Thus, the Medical Industry – as represented by the AMA (today) – will probably be against any research (like mine) – and, any proposed legislation that results – from my efforts. Thus, I propose we prepare ( now!) for their objections. I have shared my thoughts with OhiO Senator Brown - and, other Ohio politicians (as well).
I hope that you and Senator Brown can continue to work together on the Health Care issue. I appreciate that YOU – and other REPUBLICAN politicians have been brave – recently – to oppose your party leader ( Mr. Trump). Your message records will show, that I did request you to do this. OhiO Congressman Mike Turner [OH10] also did this - oppose Mr. Trump.
And, please be aware – that because (of my business experience & background) I recognize that Mr. Trump thinks – first & foremost – like a “businessman”. Thus, even he may be willing to go along – with the notion of “getting rid of medical insurance companies altogether”. Nobody likes a parasite – and, Mr. Trump – because he thinks like a “businessman” – probably hates the idea of a “parasite” on the USA Health Care system; which, from my research (thus far) – that is exactly what the Medical Insurance industry is today.
Sir, we may also need Tort reform laws – related to the USA Medical Care industry.
https://en.wikipedia.org/wiki/Universal_health_care
Universal health care, sometimes referred to as universal health coverage, universal coverage, or universal care, usually refers to a health care system that provides health care and financial protection to all citizens of a particular country. It is organized around providing a specified package of benefits to all members of a society with the end goal of providing financial risk protection, improved access to health services, and improved health outcomes.[2] Universal health care is not one-size-fits-all and does not imply coverage for all people for everything. Universal health care can be determined by three critical dimensions: who is covered, what services are covered, and how much of the cost is covered.[2] It is described by the World Health Organization as a situation where citizens can access health services without incurring financial hardship.[3] U.N. member states have agreed to work toward universal health coverage by 2030.[4]
https://en.wikipedia.org/wiki/Single-payer_healthcare
Single-payer healthcare is a healthcare system in which the state, financed by taxes, covers basic healthcare costs for all residents regardless of income, occupation, or health status. The alternatives include "multi-payer" systems in which private individuals or their employers buy health insurance or healthcare services from private or public providers.[1][2][3]
Single-payer systems may contract for healthcare services from private organizations (as is the case in Canada) or may own and employ healthcare resources and personnel (as is the case in the United Kingdom). "Single-payer" describes the mechanism by which healthcare is paid for by a single public authority, not the type of delivery or for whom physicians work. In contrast, multi-payer healthcare uses a mixed public-private system.z
https://www.democrats.org/party-platform
“ Securing Universal Health Care : Democrats believe that health care is a right, not a privilege, and our health care system should put people before profits.”
https://www.congress.gov/bill/115th-congress/house-bill/676
https://hansandcassady.org/
sssssssssssssssssssssssssssssssssssssssssssss
Senario 1 ( If needed, other scenario illustration examples will be constructed.) - Please, send me a message - by using my Contact form.
|
SCENARIO assumptions: |
( Fred and his wife ) |
|
1) Fred is a 61-year-old male.
2) Fred is a United States citizen.
3) Fred has worked - in the united States [as a "maintenance worker" ] for a "big corporation" -since he was 16-years old. Each year he has paid his personal income taxes due.
4) Fred is married - and, has been for 36+ years - and, he has two grown children. They live in California & Oregon.
5) Fred owns a modest home - in Columbus, Ohio.
6) Fred has a small sum (of cash) saved in the bank.
7) Fred & his wife have planned:
a] to sell their "paid for" home
and b] take a small vacation - after he retires.
8) Fred's wife never did (really) work outside of their home.
9) If they see a place - perhaps a condo - on their planned vacation, they may consider buying it.
10) Fred's wife's health is "good". She wants to "lose a few pounds" - she says. She goes to the YMCA - most days. She walks on the treadmill and does the "zoomba class" sometimes. She cooks breakfast, lunch & dinner - for Fred & herself - most days. She sleeps well. And, Fred finds her usually pleasant to be around.
11) Fred's health is "good" - to outward appearances; however, Fred has noticed some "shortness of breath" - when he exerts himself; and, he gets "sweaty" - unexpectedly - at times. His sleep is disturbed - some nights - by "nightmares".
12) Fred has said nothing about his "small personal issues" to his wife. (He does not want to "worry" her.)
13) Fred has "health insurance" supplied by his employer.
14) Fred wants to take the "early retirement" option - his employer has just offered him.
|



( WE ARE ALL AMERICANS ! )
|
|
|
|
( INTAKE Centers - all over the USA ) Hello! How may I help you today? You can: 1) fill out a form; 2) Talk to a computerized assistant; 3) Make an appointment - to talk with a human USA Universal Health Care "intake" professional; or, 4) Please just leave your name - and, a contact method & we will contact you.
You came in the door for "something". Let's get to it.
hhh 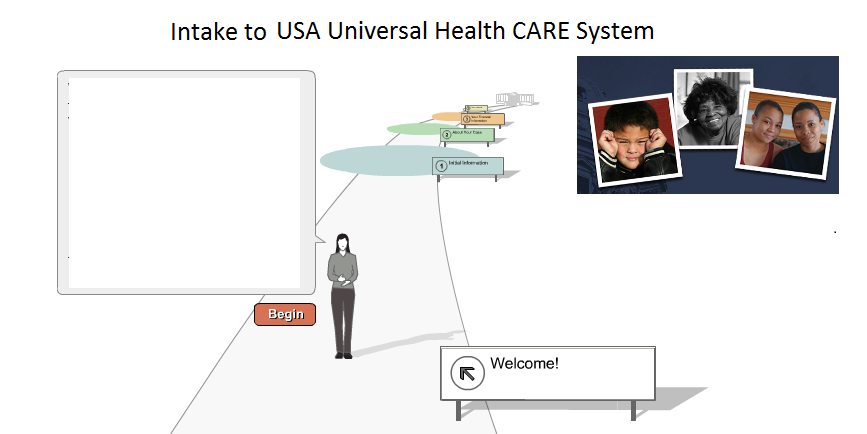 < Americans >
< Americans >
FlowChart (start) Fred has made the "first STEP" - "intake" (above) NOTE: Graphic (above) - from USA Legal Aid Society
[ DECISION POINT ] : Is "Fred's Issue" an EMERGENCY ? YES-GO A NO-GO B UNKNOWN-GO C
A ( EMERGENCY - YES )
B ( EMERGENCY - NO )
C ( EMERGENCY - UNKNOWN )
************************
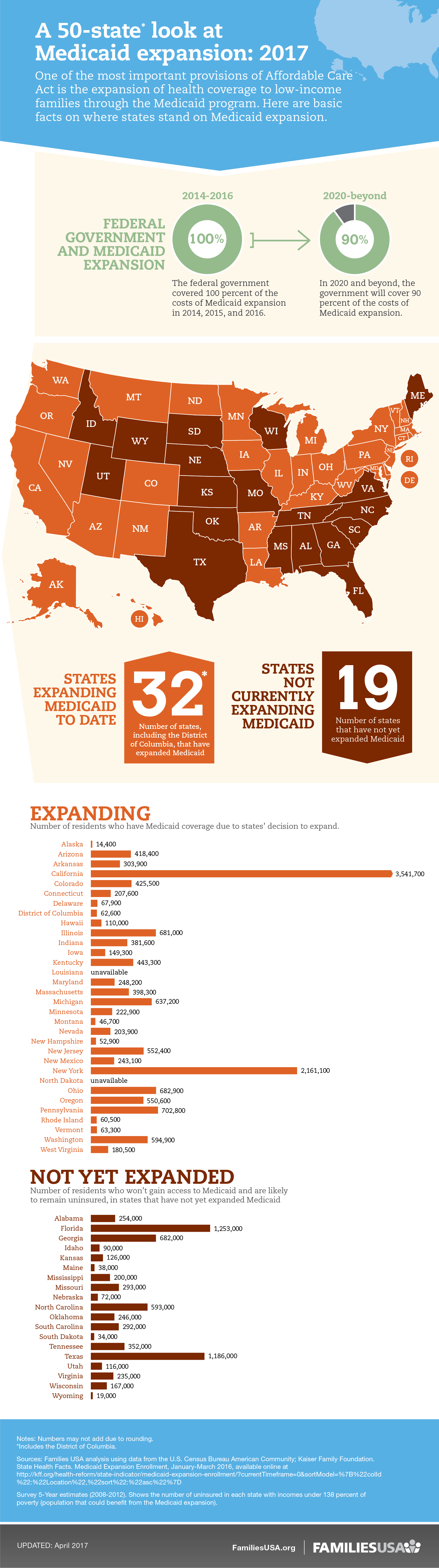
Hhhhhhhhhhhhhhhh Kaiser Chart hhhhhhhhhhhhhhhhhh
http://www.kff.org/other/state-indicator/total-population/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
Health Insurance Coverage of the Total Population
NOTES ( by Kaiser)
The majority of our health coverage topics are based on analysis of the Census Bureau’s March Supplement to the Current Population Survey (the CPS Annual Social and Economic Supplement or ASEC) by the Kaiser Commission on Medicaid and the Uninsured. The CPS supplement is the primary source of annual health insurance coverage information in the United States.
In this analysis, income (mostly categorized as a percent of the federal poverty level) is aggregated by Census-defined family units. Analyzing income by family unit captures income available to a group of people who are likely sharing resources. However, family units may not be the appropriate measure for capturing eligibility for health insurance. Eligibility for health insurance is more accurately estimated using “health insurance units,” which may be counted differently for different types of insurance (such as Medicaid or employer coverage).
Data exclude a small number of people with private coverage of an unknown source. Data may not sum to totals due to rounding and the exclusion of these people.
Sources
Kaiser Family Foundation estimates based on the Census Bureau's March 2014, March 2015, and March 2016 Current Population Survey (CPS: Annual Social and Economic Supplements).
Definitions
The ASEC asks respondents about their health insurance coverage throughout the previous calendar year. Respondents may report having more than one type of coverage. In this analysis, individuals are sorted into only one category of insurance coverage using the following hierarchy:
Medicaid: Includes those covered by Medicaid, the Children’s Health Insurance Program (CHIP), and those who have both Medicaid and another type of coverage, such as dual eligibles who are also covered by Medicare.
Medicare: Includes those covered by Medicare, Medicare Advantage, and those who have Medicare and another type of non-Medicaid coverage where Medicare is the primary payer. Excludes those with Medicare Part A coverage only and those covered by Medicare and Medicaid (dual eligibles).
Employer: Includes those covered by employer-sponsored coverage either through their own job or as a dependent in the same household.
Other Public: Includes those covered under the military or Veterans Administration.
Non-Group: Includes individuals and families that purchased or are covered as a dependent by non-group insurance.
Uninsured: Includes those without health insurance and those who have coverage under the Indian Health Service only.
For example, a person having Medicaid coverage in the first half of the year but employer-based coverage in the last months of the year would be categorized as having Medicaid coverage in this analysis.
N/A: Estimates with relative standard errors greater than 30% are not provided.
TAGS
CATEGORIES
********************************************** Do the math. Following idea to be highlighted & "sold" - educate
Business owners wouldn’t have to insure their workers.
Obamacare required businesses with at least 50 full-time employees to provide its workers with “affordable” insurance – essentially, insurance that cost less than 10 percent of a worker’s household income. ( < BIG "compromise" compare 1787 & "slavery compromise: also, compare "Patton" wanted to "handle" the Communists - when he was there. )
Failure to do that currently costs business owners up to $2,260 per employee annually. That tax penalty would disappear under the GOP plan. ( OR, it would "disappear" with a "National Single-Payer" system.)
So if a person owned a medium-sized business, and didn’t want to provide insurance, she or he could stop.
Here’s the thing: This penalty didn’t affect most “small business” owners.
Of the nearly 30 million businesses in the U.S., 80 percent have no employees – the proprietor is the only one in the shop, according to Small Business Administration data from 2013.
Many medium-sized businesses already provided insurance for their workers before Obamacare took effect.
So while some may be glad that they can stop, others are wondering how the GOP health plan will affect insurance rates. Will they be able to afford their employees’ insurance?
Currently, 52 percent of Ohioans get their insurance through an employer, compared with only 5 percent who get private insurance on the Obamacare exchange, according to Kaiser data.
http://www.cincinnati.com/story/news/politics/2017/03/11/5-ways-house-gop-health-plan-would-affect-ohioans/98987230/ <source
http://www.kff.org/other/state-indicator/total-population/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
|
|
|
|
|
|
|
|
|
|
Health Insurance |
Insurance Coverage |
Insurance Premium |
Expense |
Adjusted Gross Income - AGI |
Deductible |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HEALTH-CARE PROFITEERING profit sick people illness < Googled
https://www.forbes.com/sites/peterubel/2014/02/12/is-the-profit-motive-ruining-american-healthcare/#315aad4637b9
http://www.vanityfair.com/news/2009/09/health-care200909
Health Insurance Copied ‘originally FROM: http://www.investopedia.com/terms/h/healthinsurance.asp?lgl=myfinance-layout-no-ads Date of copy: 6-27-2017
By Investopedia Staff ( Susan is preparing a PDF document - that will list "Investopedia Staff" [ the human beings ] by name ) The following has been edited - by Susan.
What is 'Health Insurance'
Health insurance is a type of insurance coverage that pays for medical and surgical expenses incurred by the insured. Health insurance can:
- reimburse the insured for expenses incurred from illness or injury, or
2) pay the care provider directly.
It is often included in employer benefit packages as a means of enticing or retaining quality employees.
The cost of health insurance premiums is deductible to the payer, and benefits received are tax-free.
(As seen above "Health insurance" companies make "billions" of dollars - each year - for their investor "Owners".)
Thus, Susan ask: Why do we need insurance companies - at all? )
BREAKING DOWN 'Health Insurance'
THERE ARE DIFFERENT TYPE OF “HEALTH INSURANCE” PROGRAMS:
Managed care insurance plans (MCIP) - are ONE of the types.
A] MCIP require policy holders to receive care from a network of designated health care providers for the highest level of coverage.
B] If patients seek care outside the MCIP network, they must pay a higher percentage of the cost.
C] In some cases, the MCIP may refuse payment outright for services “obtained out of network”. Many MCIPs require patients to choose a “ primary care physician “ who oversees the patient's care and makes recommendations about treatment.
D) MCIP Insurance companies may also deny coverage for services that were obtained without pre - authorization.
E) In addition, MCIP insurers may refuse payment for name brand drugs if a generic version or comparable medication is available at a lower cost.
MCIPs (with higher out-of-pocket costs) generally have smaller monthly premiums than plans with low deductibles.
Affordable Care Act
In 2010, President Barack Obama signed the “Patient Protection and Affordable Care Act “ into law.
The ACA prohibits insurance companies from:
1) denying coverage to patients with pre-existing conditions,
2) and allows children to remain on their parents' insurance plan until they reach the age of 26.
3) In participating states, the act also expanded Medicaid, a government program that provides medical care for individuals with very low incomes.
4) In addition to these changes, the ACA established the “federal Healthcare Marketplace”. The “marketplace” helps individuals and businesses shop for quality insurance plans at affordable rates. Low-income individuals who sign up for insurance through the marketplace may qualify for subsidies to help bring down costs.
Under ACA Americans are required to carry medical insurance ( that meets “federally designated minimum standards” ) or face a tax penalty.
In certain cases, taxpayers may qualify for an exemption from the penalty - if they were unable to obtain insurance due to financial hardship or other situations.
[ END of copy ]
MORE RESEARCH
Sent: 6-27-2017
"Hello. I am preparing a document - for posting to my personal web site ( https://hansandcassady.org/ ). The topic is: WHY do we need Medical Insurance Companies ( at all )?
I am a supporter of Congressman John Conyer's Bill HR676. I currently believe that HR676 can be improved - by eliminating Health Care - Insurance companies - alltogether.
I believe that Americans should pay into a central system [instead] - such as Social Security - and, the funds collected would be used to fund USA Universal Health Care.
Thus, eliminating - the "middle-man" of insurance companies. I do NOT wish to harm your good efforts.
I remain an "Obama Girl" at this writing. Please suggest any reading material - to me ( by email)- that you feel may be helpful - or, informative to me."
https://questions.cms.gov/newrequest.php
history Medical Insurance
https://www.cms.gov/About-CMS/About-CMS.html
https://marketplace.cms.gov/ < official Marketplace
https://www.healthcaremarketplace.com/
https://www.healthcaremarketplace.com/about_us?on=L1auZSXy_pcrid_organic-HCMP-
http://pnhp.org/blog/2016/11/28/our-profiteering-health-insurance-industry-should-the-government-bail-it-out-again/
https://www.forbes.com/sites/peterubel/2014/02/12/is-the-profit-motive-ruining-american-healthcare/#315aad4637b9
HEALTH-CARE PROFITEERING < Google
http://www.vanityfair.com/news/2009/09/health-care200909
profit sick people illness < Googled
https://en.wikipedia.org/wiki/Health_insurance_in_the_United_States#History :: During the 1920s, individual hospitals began offering services to individuals on a pre-paid basis, eventually leading to the development of Blue Cross organizations in the 1930s. The first employer-sponsored hospitalization plan was created by teachers in Dallas, Texas in 1929.
https://en.wikipedia.org/wiki/Health_insurance_in_the_United_States
“ communal interests “ “risk sharing” Health Care < Googled
https://www.help.senate.gov/imo/media/Risk_Sharing.pdf
Ely Times column: Individual rights vs. communal interests
Insurance Coverage
What is 'Insurance Coverage'
Insurance coverage is the amount of risk or liability that is covered for an individual or entity by way of insurance services.
Insurance coverage, such as auto insurance, life insurance – or more exotic forms, such as hole-in-one insurance – is issued by an insurer in the event of unforeseen occurrences.
BREAKING DOWN 'Insurance Coverage'
Insurance coverage helps consumers recover financially from unexpected events, such as car accidents or the loss of an income-producing adult supporting a family.
Insurance coverage COST is often determined by multiple factors. In Medical Insurance, the factors are: X, Y, Z
Insurance Premium
By Brent Radcliffe www.investopedia.com/contributors/242/
What is 'Insurance Premium'
An insurance premium is the amount of money that an individual or business must pay for an insurance policy. The insurance premium is considered income by the insurance company once it is earned, and also represents a liability in that the insurer must provide coverage for claims being made against the policy.
BREAKING DOWN 'Insurance Premium'
The amount of insurance premium that is required for insurance coverage depends on a variety of factors. Insurance companies examine
the type of coverage,
the likelihood of a claim being made,
the area where the policyholder lives or operates a business,
the behavior of the person or business being covered,
and the amount of competition that the insurer faces.
[[ https://en.wikipedia.org/wiki/Actuary ]] < Good INSURANCE History section - BASICALLY, WHY we have insurance - the concept.
Actuaries employed by an insurance company can determine, for example, the likelihood of a claim being made against a teenage driver living in an urban area compared to one in a suburban area. In general, the greater the risk associated with a policy the more expensive the insurance policy will be.
Policyholders are often given a number of options when it comes to paying an insurance premium. Some insurers allow the policyholder to pay the insurance premium in installments, for example monthly or semi-annual payments, or may require the policyholder to pay the total amount before coverage starts.
Insurance premiums may increase after the policy period ends. The insurer may increase the premium if claims were made during the previous period, if the risk associated with offering a particular type of insurance increases, or if the cost of providing coverage increases.
Insurers use the insurance premium to cover the liabilities associated with the policies that they underwrite, as well as to invest the premium in order to generate higher returns. Insurers will invest the premiums in assets with varying levels of liquidity and return, with the amount of liquid assets often set by state insurance regulators. Regulators want to make sure that policyholders will be able to have their claims paid for, and thus require insurers to retain adequate reserves.
Expense --What is an 'Expense'
An expense consists of the economic costs a business incurs through its operations to earn revenue. Businesses are allowed to write off tax-deductible expenses on their income tax returns to lower their taxable income and thus their tax liability. Common business expenses include payments to suppliers, employee wages, factory leases and equipment depreciation, but the Internal Revenue Service has strict rules on which expenses business are allowed to claim as a deduction.
BREAKING DOWN 'Expense'
The term "expense" also operates as a verb, and it means to write off an expense. For example, a freelance writer may expense the cost of buying writing utensils for his business, or the executive may expense the cost of taking his clients to dinner because the group discussed business at the table.
Deductible Business Expenses
According to the IRS, to be deductible, a business expense must be both ordinary and necessary. Ordinary means the expense is common or accepted in that industry, while necessary means the expense is helpful in the pursuit of earning income. Business owners are not allowed to claim their personal, nonbusiness expenses as business deductions.
Recording Expenses
Accountants record expenses through one of two accounting methods: cash basis or accrual basis. Under cash basis accounting, expenses are recorded when they are paid. For example, if a business owner schedules a carpet cleaner to clean the carpets in his office and the cleaner invoices the company for the service, a company using cash basis records the expense when it pays the invoice. Under the accrual method, however, expenses are recorded when they are incurred, and to continue with the above example, the business accountant records the carpet cleaning expense when the company receives the service.
Capital Expenses
The IRS treats capital expenses differently than most other business expenses. While most costs of doing business can be expensed or written off against business income the year they are incurred, capital expenses must be capitalized or written off incrementally.
Capital expenses are typically large expenditures considered investments into a company. They include business startup costs; business assets such as real estate, vehicles, equipment and patents; and improvements such as putting a new HVAC system into a building. Rather than writing off these expenses in the year they are incurred, business owners must write them off slowly over time. The IRS has a schedule that dictates the portion of a capital asset a business may write off each year until the entire expense is claimed. The number of years over which a business writes off a capital expense varies based on the type of asset.
Adjusted Gross Income - AGI
What is 'Adjusted Gross Income - AGI'
Adjusted gross income (AGI) is a measure of income calculated from your gross income and used to determine how much of your income is taxable.
BREAKING DOWN 'Adjusted Gross Income - AGI'
Adjusted gross income (AGI) is a modification of gross income in the United States tax code. Gross income is simply the sum of everything an individual earns in a year. AGI factors a number of deductions from one's gross income to reach the figure for which an individual's income taxes will be calculated, and is generally more useful than gross income for individual tax activities. The deductions which modify gross income to adjusted gross income are all above the line, which means that they are taken into account before tax exemptions for military service, dependent status, etc.
Some of the most prominent deductions made to reach an individual's adjusted gross income include
- Un - reimbursed business expenses
- Medical expenses
- Alimony
- Retirement plan contributions
- Losses incurred from the sale or exchange of property
When calculating individual AGI, begin by tallying your reported income statements for the year in question, while also adding other sources of taxable income: profit on the sale of property, unemployment compensation, pensions, Social Security payments and any other income not reported on your tax returns. From this total of earnings, subtract the applicable deductions to reach your AGI. A complete list of the requirements for possible deductions from gross income can be found in the Internal Revenue Code or on the IRS website. Many of the requirements are very specific, and an individual must look very carefully at the federal tax code to make sure they are eligible for any deductions they are making.
After calculating AGI, the taxpayer can then apply the standard federal tax deductions to reach their taxable income, or if eligible, the taxpayer can itemize their expenses and receive itemized deductions instead, which can be better for the taxpayer in some situations. When working on individual taxes, then, the AGI is an important but intermediate step in determining how much of one's gross income is taxable. Be careful not to confuse AGI with modified adjusted gross income (MAGI), which is used to calculate an individual's deductible amount from an individual retirement account (IRA).
Deductible - A deductible is the amount of money an individual pays for expenses before his insurance plan starts to pay.
The word "deductible" can also work as an adjective to describe the tax-deductible expenses that can deducted from someone's adjusted gross income to reduce his taxable income and his tax liability.
BREAKING DOWN 'Deductible'
To understand insurance deductibles, imagine your deductible is $300, and you incur medical expenses for $2,000. You pay the $300 deductible, also called the out-of-pocket cost, and your insurer pays the remaining $1,700. However, if your entire medical bill is $300, you would pay the entire amount and your insurer would pay nothing.
Insurance deductibles do not just apply to health insurance. Car insurance, homeowners insurance, renters insurance and other types of insurance policies also have deductibles. In the United Kingdom, Australia and some other parts of the world, an insurance deductible is referred to as an excess, but excesses and deductibles function in the same way.
Tax Deductible Expenses
The Internal Revenue Service (IRS) considers a number of expenses to be tax-deductible. To reduce their taxable income, tax filers may deduct eligible healthcare expenses, mortgage interest expenses and some investment-related expenses. However, for those with brokerage accounts, fees such as commissions paid for trades are not deductible.
The IRS divides tax deductible expenses or deductions into two major categories: individual and business.
Deductible Expenses for Individuals
Individuals may claim a standard deduction based on their marital status, filing status and number of children. Set by the IRS and reviewed annually, the standard deduction is subject to change, but as of 2016, it is $6,300 for an individual. If an individual reports $40,000 in taxable income, for example, he can then deduct $6,300 to lower his taxable income to $33,700.
In lieu of the standard deduction, tax filers may opt to itemize their deductions. This means they add together the value of a long list of deductions and then subtract that amount from their earnings to determine their taxable income. Examples of itemized deductions include charitable contributions, mortgage interest, and medical and dental expenses.
Business Deductions
Business deductions work slightly differently from individual deductions. If a small business owner, a self-employed individual, an independent contractor or a corporation is filing taxes, the tax filer reports all of the income the business receives during the tax year. Then, he deducts business expenses from that amount. The difference is the business's taxable income. Deductible business expenses include operating expenses such as payroll, utilities, rent, leases and other costs of running the business. Capital expenses such as buying equipment or real estate for the business are also deductible.
Health Insurance Cut FROM: http://www.investopedia.com/terms/h/healthinsurance.asp?lgl=myfinance-layout-no-ads Date of copy: 6-27-2017
By Investopedia Staff ( Susan is preparing a PDF document - that will list "Investopedia Staff" [ the human beings ] by name ) The following has been edited - by Susan.
What is 'Health Insurance'
Health insurance is a type of insurance coverage that pays for medical and surgical expenses incurred by the insured. Health insurance can reimburse the insured for expenses incurred from illness or injury, or pay the care provider directly. It is often included in employer benefit packages as a means of enticing quality employees. The cost of health insurance premiums is deductible to the payer, and benefits received are tax-free.
BREAKING DOWN 'Health Insurance'
Managed care insurance plans require policy holders to receive care from a network of designated health care providers for the highest level of coverage. If patients seek care outside the network, they must pay a higher percentage of the cost. In some cases, the insurance company may even refuse payment outright for services obtained out of network. Many managed care plans require patients to choose a primary care physician who oversees the patient's care and makes recommendations about treatment. Insurance companies may also deny coverage for services that were obtained without pre - authorization. In addition, insurers may refuse payment for name brand drugs if a generic version or comparable medication is available at a lower cost.
Insurance plans with higher out-of-pocket costs generally have smaller monthly premiums than plans with low deductibles. When shopping for plans, individuals must weigh the benefits of lower monthly costs against the potential risk of large out-of-pocket expenses in the case of a major illness or accident. Health insurance has many cousins, such as disability insurance, critical (catastrophic) illness insurance and long-term care (LTC) insurance.
Affordable Care Act
In 2010, President Barack Obama signed the Patient Protection and Affordable Care Act into law. It prohibits insurance companies from denying coverage to patients with pre-existing conditions, and allows children to remain on their parents' insurance plan until they reach the age of 26. In participating states, the act also expanded Medicaid, a government program that provides medical care for individuals with very low incomes. In addition to these changes, the ACA established the federal Healthcare Marketplace. The marketplace helps individuals and businesses shop for quality insurance plans at affordable rates. Low-income individuals who sign up for insurance through the marketplace may qualify for subsidies to help bring down costs.
Americans are required to carry medical insurance that meets federally designated minimum standards or face a tax penalty. In certain cases, taxpayers may qualify for an exemption from the penalty if they were unable to obtain insurance due to financial hardship or other situations. Two public health insurance plans, Medicare and the Children's Health Insurance Program, target older individuals and children, respectively. Medicare also serves people with certain disabilities. The program is available to anyone age 65 or older. The CHIP plan has income limits and covers babies and children up to the age of 18.
[ END of copy ]
Insurance Coverage
What is 'Insurance Coverage'
Insurance coverage is the amount of risk or liability that is covered for an individual or entity by way of insurance services. Insurance coverage, such as auto insurance, life insurance – or more exotic forms, such as hole-in-one insurance – is issued by an insurer in the event of unforeseen occurrences.
BREAKING DOWN 'Insurance Coverage'
Insurance coverage helps consumers recover financially from unexpected events, such as car accidents or the loss of an income-producing adult supporting a family.
Insurance coverage is often determined by multiple factors. For example, most insurers charge higher premiums for young male drivers, as insurers deem the probability of young men being involved in accident to be higher than say, a middle-aged married man with years of driving experience.
Auto Insurance Coverage [ comparison of how price is determined ]
Auto insurance premiums depend on the insured party's driving record. A record free of accidents or serious traffic violations typically results in a lower premium. Drivers with histories of accidents or serious traffic violations may pay higher premiums. Likewise, because mature drivers tend to have fewer accidents than less-experienced drivers, insurers typically charge more for drivers below age 25.
Insurance Premium
By Brent Radcliffe www.investopedia.com/contributors/242/
What is 'Insurance Premium'
An insurance premium is the amount of money that an individual or business must pay for an insurance policy. The insurance premium is considered income by the insurance company once it is earned, and also represents a liability in that the insurer must provide coverage for claims being made against the policy.
BREAKING DOWN 'Insurance Premium'
The amount of insurance premium that is required for insurance coverage depends on a variety of factors. Insurance companies examine the type of coverage, the likelihood of a claim being made, the area where the policyholder lives or operates a business, the behavior of the person or business being covered, and the amount of competition that the insurer faces.
[[ https://en.wikipedia.org/wiki/Actuary ]]
Actuaries employed by an insurance company can determine, for example, the likelihood of a claim being made against a teenage driver living in an urban area compared to one in a suburban area. In general, the greater the risk associated with a policy the more expensive the insurance policy will be.
Policyholders are often given a number of options when it comes to paying an insurance premium. Some insurers allow the policyholder to pay the insurance premium in installments, for example monthly or semi-annual payments, or may require the policyholder to pay the total amount before coverage starts.
Insurance premiums may increase after the policy period ends. The insurer may increase the premium if claims were made during the previous period, if the risk associated with offering a particular type of insurance increases, or if the cost of providing coverage increases.
Insurers use the insurance premium to cover the liabilities associated with the policies that they underwrite, as well as to invest the premium in order to generate higher returns. Insurers will invest the premiums in assets with varying levels of liquidity and return, with the amount of liquid assets often set by state insurance regulators. Regulators want to make sure that policyholders will be able to have their claims paid for, and thus require insurers to retain adequate reserves.
Expense
What is an 'Expense'
An expense consists of the economic costs a business incurs through its operations to earn revenue. Businesses are allowed to write off tax-deductible expenses on their income tax returns to lower their taxable income and thus their tax liability. Common business expenses include payments to suppliers, employee wages, factory leases and equipment depreciation, but the Internal Revenue Service has strict rules on which expenses business are allowed to claim as a deduction.
BREAKING DOWN 'Expense'
The term "expense" also operates as a verb, and it means to write off an expense. For example, a freelance writer may expense the cost of buying writing utensils for his business, or the executive may expense the cost of taking his clients to dinner because the group discussed business at the table.
Deductible Business Expenses
According to the IRS, to be deductible, a business expense must be both ordinary and necessary. Ordinary means the expense is common or accepted in that industry, while necessary means the expense is helpful in the pursuit of earning income. Business owners are not allowed to claim their personal, nonbusiness expenses as business deductions.
Recording Expenses
Accountants record expenses through one of two accounting methods: cash basis or accrual basis. Under cash basis accounting, expenses are recorded when they are paid. For example, if a business owner schedules a carpet cleaner to clean the carpets in his office and the cleaner invoices the company for the service, a company using cash basis records the expense when it pays the invoice. Under the accrual method, however, expenses are recorded when they are incurred, and to continue with the above example, the business accountant records the carpet cleaning expense when the company receives the service.
Capital Expenses
The IRS treats capital expenses differently than most other business expenses. While most costs of doing business can be expensed or written off against business income the year they are incurred, capital expenses must be capitalized or written off incrementally.
Capital expenses are typically large expenditures considered investments into a company. They include business startup costs; business assets such as real estate, vehicles, equipment and patents; and improvements such as putting a new HVAC system into a building. Rather than writing off these expenses in the year they are incurred, business owners must write them off slowly over time. The IRS has a schedule that dictates the portion of a capital asset a business may write off each year until the entire expense is claimed. The number of years over which a business writes off a capital expense varies based on the type of asset.
Adjusted Gross Income - AGI
What is 'Adjusted Gross Income - AGI'
Adjusted gross income (AGI) is a measure of income calculated from your gross income and used to determine how much of your income is taxable.
BREAKING DOWN 'Adjusted Gross Income - AGI'
Adjusted gross income (AGI) is a modification of gross income in the United States tax code. Gross income is simply the sum of everything an individual earns in a year. AGI factors a number of deductions from one's gross income to reach the figure for which an individual's income taxes will be calculated, and is generally more useful than gross income for individual tax activities. The deductions which modify gross income to adjusted gross income are all above the line, which means that they are taken into account before tax exemptions for military service, dependent status, etc.
Some of the most prominent deductions made to reach an individual's adjusted gross income include
- Un - reimbursed business expenses
- Medical expenses
- Alimony
- Retirement plan contributions
- Losses incurred from the sale or exchange of property
When calculating individual AGI, begin by tallying your reported income statements for the year in question, while also adding other sources of taxable income: profit on the sale of property, unemployment compensation, pensions, Social Security payments and any other income not reported on your tax returns. From this total of earnings, subtract the applicable deductions to reach your AGI. A complete list of the requirements for possible deductions from gross income can be found in the Internal Revenue Code or on the IRS website. Many of the requirements are very specific, and an individual must look very carefully at the federal tax code to make sure they are eligible for any deductions they are making.
After calculating AGI, the taxpayer can then apply the standard federal tax deductions to reach their taxable income, or if eligible, the taxpayer can itemize their expenses and receive itemized deductions instead, which can be better for the taxpayer in some situations. When working on individual taxes, then, the AGI is an important but intermediate step in determining how much of one's gross income is taxable. Be careful not to confuse AGI with modified adjusted gross income (MAGI), which is used to calculate an individual's deductible amount from an individual retirement account (IRA).
Deductible
A deductible is the amount of money an individual pays for expenses before his insurance plan starts to pay.
The word "deductible" can also work as an adjective to describe the tax-deductible expenses that can deducted from someone's adjusted gross income to reduce his taxable income and his tax liability.
BREAKING DOWN 'Deductible'
To understand insurance deductibles, imagine your deductible is $300, and you incur medical expenses for $2,000. You pay the $300 deductible, also called the out-of-pocket cost, and your insurer pays the remaining $1,700. However, if your entire medical bill is $300, you would pay the entire amount and your insurer would pay nothing.
Insurance deductibles do not just apply to health insurance. Car insurance, homeowners insurance, renters insurance and other types of insurance policies also have deductibles. In the United Kingdom, Australia and some other parts of the world, an insurance deductible is referred to as an excess, but excesses and deductibles function in the same way.
Tax Deductible Expenses
The Internal Revenue Service (IRS) considers a number of expenses to be tax-deductible. To reduce their taxable income, tax filers may deduct eligible healthcare expenses, mortgage interest expenses and some investment-related expenses. However, for those with brokerage accounts, fees such as commissions paid for trades are not deductible.
The IRS divides tax deductible expenses or deductions into two major categories: individual and business.
Deductible Expenses for Individuals
Individuals may claim a standard deduction based on their marital status, filing status and number of children. Set by the IRS and reviewed annually, the standard deduction is subject to change, but as of 2016, it is $6,300 for an individual. If an individual reports $40,000 in taxable income, for example, he can then deduct $6,300 to lower his taxable income to $33,700.
In lieu of the standard deduction, tax filers may opt to itemize their deductions. This means they add together the value of a long list of deductions and then subtract that amount from their earnings to determine their taxable income. Examples of itemized deductions include charitable contributions, mortgage interest, and medical and dental expenses.
Business Deductions
Business deductions work slightly differently from individual deductions. If a small business owner, a self-employed individual, an independent contractor or a corporation is filing taxes, the tax filer reports all of the income the business receives during the tax year. Then, he deducts business expenses from that amount. The difference is the business's taxable income. Deductible business expenses include operating expenses such as payroll, utilities, rent, leases and other costs of running the business. Capital expenses such as buying equipment or real estate for the business are also deductible.
http://www.kff.org/other/state-indicator/total-population/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
Health Insurance Coverage of the Total Population
NOTES ( by Kaiser)
The majority of our health coverage topics are based on analysis of the Census Bureau’s March Supplement to the Current Population Survey (the CPS Annual Social and Economic Supplement or ASEC) by the Kaiser Commission on Medicaid and the Uninsured. The CPS supplement is the primary source of annual health insurance coverage information in the United States.
In this analysis, income (mostly categorized as a percent of the federal poverty level) is aggregated by Census-defined family units. Analyzing income by family unit captures income available to a group of people who are likely sharing resources. However, family units may not be the appropriate measure for capturing eligibility for health insurance. Eligibility for health insurance is more accurately estimated using “health insurance units,” which may be counted differently for different types of insurance (such as Medicaid or employer coverage).
Data exclude a small number of people with private coverage of an unknown source. Data may not sum to totals due to rounding and the exclusion of these people.
Sources
Kaiser Family Foundation estimates based on the Census Bureau's March 2014, March 2015, and March 2016 Current Population Survey (CPS: Annual Social and Economic Supplements).
Definitions
The ASEC asks respondents about their health insurance coverage throughout the previous calendar year. Respondents may report having more than one type of coverage. In this analysis, individuals are sorted into only one category of insurance coverage using the following hierarchy:
Medicaid: Includes those covered by Medicaid, the Children’s Health Insurance Program (CHIP), and those who have both Medicaid and another type of coverage, such as dual eligibles who are also covered by Medicare.
Medicare: Includes those covered by Medicare, Medicare Advantage, and those who have Medicare and another type of non-Medicaid coverage where Medicare is the primary payer. Excludes those with Medicare Part A coverage only and those covered by Medicare and Medicaid (dual eligibles).
Employer: Includes those covered by employer-sponsored coverage either through their own job or as a dependent in the same household.
Other Public: Includes those covered under the military or Veterans Administration.
Non-Group: Includes individuals and families that purchased or are covered as a dependent by non-group insurance.
Uninsured: Includes those without health insurance and those who have coverage under the Indian Health Service only.
For example, a person having Medicaid coverage in the first half of the year but employer-based coverage in the last months of the year would be categorized as having Medicaid coverage in this analysis.
N/A: Estimates with relative standard errors greater than 30% are not provided.
TAGS
CATEGORIES
Hhhhhhhhhhhhhhh Democrat’s platform hhhhhhhhhhhhhhhh
Securing Universal Health Care
Democrats believe that health care is a right, not a privilege, and our health care system should put people before profits.
Thanks to the hard work of President Obama and Democrats in Congress, we took a critically important step toward the goal of universal health care by passing the Affordable Care Act, which has covered 20 million more Americans and ensured millions more will never be denied coverage because of a pre-existing condition.
Democrats will never falter in our generations-long fight to guarantee health care as a fundamental right for every American.
As part of that guarantee, Americans should be able to access public coverage through a public option, and those over 55 should be able to opt in to Medicare.
Democrats will fight any attempts by Republicans in Congress to privatize, voucherize, or “phase out” Medicare as we know it.
We will keep fighting until the ACA’s Medicaid expansion has been adopted in every state.
Nineteen states have not yet expanded Medicaid. This means that millions of low-income Americans still lack health insurance and are not getting the care they need. Additionally, health care providers, clinics, hospitals, and taxpayers are footing a higher bill when people without insurance visit expensive emergency rooms.
Supporting Community Health Centers
We must renew and expand our commitment to Community Health Centers, as well as community mental health centers and family planning centers. These health centers provide critically important, community-based prevention and treatment in underserved communities, prevent unnecessary and expensive trips to emergency rooms, and are essential to the successful implementation of the ACA.
We will fight for a comprehensive system of primary health care, including dental, mental health care, and low-cost prescription drugs by doubling of funding for federally qualified community health centers over the next decade, which currently serve 25 million people.
Democrats also know that one of the key ingredients to the success of these health centers is a well-supported and qualified workforce in community-based settings.
We will fight to train and support this workforce, encourage providers to work with underserved populations through the National Health Service Corps, and create a comprehensive strategy to increase the pool of primary health care professionals.
.
Democrats are committed to investing in the research, development, and innovation that creates lifesaving drugs and lowers overall health costs, but the profiteering of pharmaceutical companies is simply unacceptable.
Hhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhh
> Hello World ! YOU have reached
the personal web site of Susan Marie Cassady-Neuhart.
|
The American Health Act ( AHA) ...
|
|
|
Susan's last UP-DATE: 4-13-2017!
( FSMB ) < Please read this first - to understand "how" the debate is - and, will be (for ever) - informed by "Medical Professionals" - and, their representatives.
The Tenth Amendment to the United States Constitution authorizes states to establish laws and regulations protecting the health, safety and general welfare of their citizens.[6]
Required REFORM of - Medical Liability Insurance market & industry : ( REPORT [pdf] - dated September 12, 2004 ) < Please read report to find the reasons & history - for the current system - of health care - and, its related current pricing - to American consumers.
The American Health Act ( AHA)
( - from "Obama Care" to "Trump Care" )
[ Susan's "idea" text follows ]
The following is Susan's idea ( text only)! This is NOT a bill - or anything official.
YES! - I did try to read the "official" document (links above); However, to "me" - a person with much practical experience ( 30+ years) in reading many complicated, software engineering documents - it ( the official Bill ) is unintelligible. I only know that - it appears ( to "me") - THEY are allotting - more than $15-Billion dollars (in HR 1628) - for something; and, insurance companies, are prominently mentioned ( I feel ) - to receive a large portion of these tax payer funds - with no practical over-sight (detailed) insofar as how they ( the Medical Insurance companies) will further distribute these funds.
The American Health Act ( AHA)
( - from Obama Care to Trump Care )
If agreed to - by Mr. Trump: On May 31, 2017, the American Health Act [ AHA ] shall be introduced by the Donald J. Trump Presidential Administration. The AHA (Act) shall be passed unanimously by the US Congress and receive a Presidential signature - within 2 business days.
President Franklin D. Roosvelt passed such sweeping legislation - during his presidency - And, similar to today - the times and the conditions warranted this.
https://millercenter.org/president/fdroosevelt/domestic-affairs
Key features of the AHA:
- The primary objective of the Act is to protect, promote and restore the physical and mental well-being of citizens of the USA - and, to facilitate reasonable access to health services - through out America - without financial, physical or other barriers. We are all Americans. And, America is a great country. This ACT takes a step to re-claim our international heritage - as a world-leader in all things.
- Another objective of the American Health Act is: continued access to quality health care - without financial or other barriers - for all Americans; as this will be critical to maintaining and improving the health and well-being of all Americans - during any transition from "Obama Care" to "Trump Care".
- To do so, the AHA shall list a set of criteria and conditions (drafted below) that each state - in our Union of 50 States - must follow in order to receive Federal Transfer Payments ( FTPs ). They are - briefly: A) Public Administration - by States, B) Comprehensiveness & Universality, C)Portability, D) Accessibility - and E) Penalties.
- Additional criteria and conditions - extending and altering this AHA - may be introduced into the US Congress (after May 31, 2017) for voting upon by the elected representatives of the American people - as conditions and experience - with the enacted AHA - warrant.
The criteria & conditions - to be met by each state AHA provider are as follows:
A) Public administration
- All AHA medical and health related services and entities must be "administered" and "operated" on a non-profit basis by licensed Medical Professionals - responsible (only) to US State governments and their medical peers.
- The "entities" administered and operated are subject to audits of their records, accounts and financial transactions - by State Government and AHA officials.
- Elimination: All so-called and in reality "Private Insurance Companies & Carriers" shall be eliminated (by this ACT) - until time and experience provides sufficient proof they are necessary - for any practical reason. That is, no one should benefit from the pain and suffering - of an American citizen.
- An ACT of the US Congress - shall be necessary to reverse the previous provision of "elimination".
B) Comprehensiveness & Universality
- There shall be no such entity - in the United States of America - as a "non-insured citizen".
- That is, every United States citizen (born and living) shall be covered and cared for - by reasonably re-numerated Medical Professionals.
- All AHA services shall be provided in excellent "World Class" American Medical Facilities - as required and needed - with no apportionment - related to a State's individual wealth or population.
- The AHA shall cover all health services provided by Medical Professionals in these facilities ( in every state) - including (as needed) psychiatry and dentistry.
- The fees (for AHA services) that may be charged - by Medical Professionals - are as described and stated in the current published USA Medicare program documents (2017).
- If Medical Professionals wish to offer services - that are not currently described by USA Medicare program documents - they may do so; however, those "additional services" shall be provided on a private business basis - and, not covered or administered by the AHA; however, all FDA & USHHS rules and regulations shall apply & be enforced.
- No Medical Professional (employed to provide services - under the AHA) - shall be permitted to simultaneously provide private business services.
- The states are permitted, to offer additional "distinguishing" medical and dental services; however, these "additional services" shall be paid for exclusively by State Transfer Payments (STPs). These STPs shall be administered by the States - and, they may not be made fungible - or, made a part of the AHA ( FTP) funds - in any manner.
C) Portability
- States shall be responsible for their state citizens - who are temporarily in another state - for purposes of work, travel, visiting, etc.
- "Temporary" from more "permanent" relocation status shall be determined - using 90 days as a standard maximum - to make the distinction ( of permanent versus temporary resident) at the program's start.
D) Accessibility
- The AHA shall provide Medical Professionals with the means to provide uniform "reasonable access" to services offered for USA citizens - using all modes of public USA transportation systems ( including trains, plains, buses, taxis, etc.) on uniform terms and conditions.
- Medical Professionals ( after licensure) shall be at liberty to "move about" in America - and, subsequently licensed in other US states.
- All AHA services shall be provided in similar and comparable "World Class" medical facilities - located in every state in America.
- There shall be no "extra-billing" - of any American citizen - for any AHA services rendered.
- Specifically, Medical Professionals in every American location - which, they choose to be located in - shall be re-numerated - at the same AHA rate (per specialty) - adjusted only for provable State "cost-of-living" differences - which, are not "controllable" by other means - such as, medical facility offerings. ( For example, AHA Medical Facilities may provide Medical Professional dormitories, meal rooms, laundries etc.)
- AHA Medical Professional day-to-day travel expenses shall not be reimbursed - through AHA funds. This is to encourage employed AHA Medical Professionals, to live near - where they choose to work - which, will result in improved inner-city areas.
E) Penalties
- The states shall ensure recognition of the Federal Transfer Payments ( FTPs) by publically viewable documents - modeled after modern transaction receipts (on state web sites, etc.)
- States shall provide information to appointed AHA officers as requested. The AHA shall mandate a Director - with staff.
- The size and scope of the AHA "directorate" shall dictate its annual budget.
- The AHA Federally designated Director and their "staff" is entitled to request and receive specific information related to a state's AHA health care services.
- This "information" shall be used in drafting AHA annual reports ( to Congress) - which shall be made available and presented to the American people - regarding how each state has administered its AHA health care services over the previous year.
- This information shall be provided on a timely basis (to the AHA staff) - on a level of detail - as requested by the AHA Federally designated "staff".
- The AHA "Director" shall be appointed by the current President of the United States (during her or his term) - and, no confirmation ( by the US Congress ) is required.
- Each AHA Director ( so named ) - shall offer their resignation - at the end of the "appointing President's" term.
- Each state must "give recognition" to the USA federal government ( as the "ultimate provider" of AHA services ) in public documents and in any advertising or promotional material, relating to Federal AHA health services in the state.
- For non-compliance - with any of the criteria listed above - the federal government ( upon proof) shall withhold all or a part of the Federal Transfer Payment.
- The federal government shall actively enforce these criteria - utilizing all eligible enforcement capabilities of its departments: DOJ, etc.
- Specifically, in recognition of the "status", "privilege" and "honor" that American society confers on licensed Medical Professionals, no Medical Professional shall a) organize "unions" or b) go on "strike" - or, c) take actions to undermine the intent of the AHA - without risk to their State and Federally granted medical license.
[ end of idea ]
|
|
|
|
|
|
|
|
|
|
|
Susan's last UP-DATE: 4-13-2017!
https://berniesanders.com/issues/medicare-for-all
Dear Mr. Sanders, the Health Plan - attributed to you ( above link ) - provides no logical or rational basis - on its face - for discussion. That is, it presents no basis for its estimated costs or the services that it provides. It states no assumptions about physicians (their numbers) - patients (their numbers) - facilities (where services will be provided) or services (what will be done). Yes, I have emailed "your representatives - as suggested - at that same web site. At this writing, I have not heard from you - or them. I look forward to moving ahead - together - and, informing each other - as we proceed. - Susan
Your representatives: Friends of Bernie Sanders
PO BOX 391
Burlington, VT 05402
email us at help@ourrevolution.com and < done !
My last UP-DATE: 4-9-2017!
( FSMB ) < Please read this first - to understand how the debate is - and, will be - informed by "Medical Professionals".
Required REFORM of - Medical Liability Lnsurance market & industry
( REPORT [pdf] - dated September 12, 2004 ) < read this to find the reasons & history...
The American Health Act ( AHA) ( - from "Obama Care" to "Trump Care" ) [ Susan's "idea" text is below ]
After your REVIEW ( of my AHA "draft" idea presented below ) - please Contact "me" - with your COMMENTS. If you are basically polite - and, I can understand the good reasons - for your comments AND suggestions - I may incorporate your comments. I will credit you - if I incorporate your comments/suggestions AND you give me your written permission (in your submission) - to identify you. Please provide a means for me to confirm - that your "identifying information" is real. Please be creative and thoughtful. For example, if you claim that you are (the) Mr. Donald Trump - or (the) Congressman Joe Kennedy - then, I must be able to verify that this is true. -- In fact, I would be honored to hear from all of you. In Columbus, Ohio - public schools ( 1960 - 1972 ) we were taught - that everyone's opinion matters. This was reinforced during my time at the University of Wisconsin ( UWGB ).
NOTE: Following is an "idea" presented by ( "me" ) Susan Marie CASSADY-Neuhart ( to Mr. Trump - initially - on 4-4, 2017). However, our US Congress is working on real ( and official ) legislation - related to this same subject. That is "Trump CARE" is not dead - and, the odds are - that the US 115th Congress will enact "something". Please become informed - and participate. https://rules.house.gov/ -- https://rules.house.gov/bill/115/hr-1628 (BILL Summary)
Your representatives (DEMs & REPs) they ( "they" ) really do want your input - on this subject. In fact, each one of them has a web site - and, you can Contact them - by various means [ telephone, USPS, contact Forms... ] - to let them know - what you think. They are looking for good ideas. Please "speak up". The US Congress House RULEs Committee member's contact information is shown below. If your state is not on the list - then, write to your Congressional Representative (any way).
For example - my current Congressional Representative is: Congressman Mr. Mike Turner [OH 10]. Mike is not on any Health-related committee (yet). And, ( he knows ) that I am a passionate Democrat. Mike is a Republican. But, even though our fundamental philosophies are different, he is listening. He is an American. And, this is what Americans "do". That is, we listen to each other. And, one day - he will vote. Until he "votes" - it is my job - as an American - to try to persuade him - to try to persuade other US Congressional Representatives. Mike's - Health CARE - related - legislation - currently pending: ( text of Mike's announcement ) H.R. 285 H.R. 286 H.R. 287
|
How Federal laws are made in the USA
( the process )
|
The following is an "idea" [ for comment ] and "proposed" ONLY ( PDF doc 3 pages) Public comments are being incorporated now. Please Contact "me" - a United States citizen.
- PLEASE, also review the official bill ( H.R. 1628 - American Health Care Act of 2017 -- pdf ) as it has been published by the US House of Representatives Clerk's Office. Please be aware this official "bill" is still - in progress - to become US Law. (BILL Summary) Visit the Rules Committee web site - and participate. https://rules.house.gov/
|
The US House of Representatives “Committee on Rules” ...
https://www.congress.gov
( search all active legislation
in the US Congress )
|
|
.Every Federal Law - in the USA - begins in the U.S. House of Representatives. (State laws are created by state legislatures. And, there are "local" government laws also.)
Federal laws super-cede all State laws; which, super-cede all local laws.
All Federal laws - in the United States - originate as written documents called "bills" .
"Bills" - and all USA law - begin as "ideas".
These ideas may come from a elected representative or from a citizen.
Citizens ( who have ideas for laws) can contact their Congressional Representatives to discuss their ideas - for a law.
Every US Citizen has 4 elected repesentatives. That is, 2 Senators, one US House Congressional district person - and, the US President. Your residential zip-code defines who your USA Congressional representatives are. The President - of the USA - is a representative of all American citizens.
If your Representatives [ or, any US HOUSE Representative agrees - with an idea - you propose ( to them) ], they may draft - your idea - into a written " bill ".
http://www.house.gov/representatives
US citizens must use only legal means - to persuade and convince their representatives to propose a bill. - LEGAL means of persuasion: ( UWGB )
A Bill Is formally "proposed" ( by a US House Representative) by a writing. Thus, many citizens draft the idea - for a bill (their "idea" ) - in writing. This beginning - in writing - is then ( most often ) changed & perfected ( by the citizen's representatives) - because, each bill must be "sponsored". That is, when a citizen's Representative has written a bill - that the Representative is pleased with, the Representative seeks sponsors - who will also support the bill. This is call " politics ".
Typically, the citizen's Representative talks with other Representatives about the bill ( as proposed ) in hopes of getting their support for it. US citizens often vote for - and select - their representatives - based upon how well - they are perceived - to perform "politic-ing" .
Once a bill has at least one sponsor - and, it is in written form -it is ready to be "introduced".
In the U.S. House of Representatives, a bill is "introduced" when it is placed into the "hopper" — a special box on the side of the US House of Representative clerk’s desk.
"hopper"
Only "elected" Representatives can introduce bills in the U.S. House of Representatives.
When a bill is introduced in the U.S. House of Representatives, a " bill clerk " assigns it a number that begins with H.R.
A "reading clerk" then (literally) reads (aloud) the bill (as placed into the hopper) to all the Representatives (present), and the Speaker of the House sends the bill to one of the House standing committees.
When the bill reaches it "assigned committee" the committe's members "review", "research", and "revise" the inially proposed bill and vote For or Against sending the bill back to the House floor.
If the committee members would like more information before deciding if the bill should be sent to the House floor, the bill is sent to a "subcommittee".
While in subcommittee, the bill is closely examined - and expert opinions are gathered - before it is sent back to the committee for approval.
When the committee has approved a bill, it is sent — or reported — to the House floor.
Once "reported", a bill is ready to be debated by the U.S. House of Representatives.
During the period of debate - all current US Congress Representatives (civilly) discuss the bill and explain - in US Communications mediums - why they agree or disagree with the bill - as presented.
Then, a "reading clerk" reads the bill ( again) - this time, section-by-section and the US Congress Representatives (again) may recommend changes - in writing.
When all changes have been made, the "final" bill is ready to be voted on - by US Congress House Representatives.
The number of voting representatives in the House is fixed ( by law) at no more than 435, proportionally representing the population of the 50 United States. Currently, there are five delegates representing the District of Columbia, the Virgin Islands, Guam, American Samoa, and the Commonwealth of the Northern Mariana Islands. A resident commissioner represents Puerto Rico.
There are three methods for voting on a bill in the U.S. House of Representatives:
1) Viva Voce (voice vote): The Speaker of the House asks the Representatives who support the bill to say “aye” and those that oppose it say “no". This "voice vote" may be recorded.
2) Division: The Speaker of the House asks those Representatives who support the bill to stand up and be counted, and then those who oppose the bill to stand up and be counted. This "divional vote" may be recorded - by photgraphs or cameras.
3) Recorded: Representatives record their vote using the electronic voting system. This "Recorded vote" is reported in all USA mediums of Communication.
Representatives may vote -yes, -no, or -present (if they don’t want to vote on the bill).
If a majority of the US Representatives say or select yes, the bill ( as presented - in its "final" form) passes in the U.S. House of Representatives -
And, it is then "certified" by the Clerk of the House [ in its final form ] and it is "delivered" to the U.S. Senate.
This phase of USA "law-making" is known as "referred to the Senate".
Each "referred bill" is (then) discussed in a Senate committee and then "reported" to the Senate floor to be voted on - by US Senators.
There are 100 US Senators. That is, each state has 2 Senators - per state.
Senators also may vote 3 ways. "Roll call", "Voice Vote" or "standing" Those who support the bill under consideration say “yea, yeah - or yes” - and those who oppose it say “nay - or no”; depending upon where they learned to speak English.
If a majority of the Senators "vote in the affirmative" the bill "passes" in the U.S. Senate - and, the Bill Is (then) Sent to the US President.
A bill that does not pass the senate "dies".
When a bill reaches the President's desk, he has three choices: He can:
1) Sign and pass the bill—the bill becomes a law.
2) Refuse to sign, or veto, the bill—the bill is "sent back" to the U.S. House of Representatives, along with the President’s reasons for the veto.
If the U.S. House of Representatives and the U.S. Senate still believe the bill should become a law, they can hold another vote on the bill.
If two-thirds of the House of Representatives and Senators support the bill, the President’s veto is overridden and the bill becomes a law - even if the US President has "vetoed" - or, refused to sign the law.
3) Or, the US President may do nothing; This is called a "pocket veto"; however, if Congress is in session, the bill automatically becomes law 10 days - after being placed upon the President's desk.
If Congress is not in session, the bill does not become a law.
If a bill has passed in both the U.S. House of Representatives and the U.S. Senate and has been approved by the President, or if a presidential veto has been overridden, the bill becomes a "law" and, it is codified and enforced by the Federal, State and local governments - in all of the USA.
This presentation of "How Federal laws are made in the USA" was informed by information published by the Office of the Clerk, U.S. Capitol, Room H154 - Washington, DC 20515-6601 : telephone (202) 225-7000
http://www.house.gov/representatives
http://clerk.house.gov/about/index.aspx
https://www.senate.gov/general/Features/votes.htm
|
The following is Susan's idea (only)! This is NOT a bill - or anything official. YES! - I did try to read the "official" document (links above); However, to "me" - a person with much experience in reading many complicated, software engineering documents - it ( the official Bill ) is unintelligible. I only know that - it appears - THEY are allotting - more than $15-Billion dollars (in HR 1628) - for something; and, insurance companies, are prominently mentioned ( I feel ) - to receive a large portion of these tax payer funds - with no over-sight insofar as how they ( the Medical Insurance companies) further distribute these funds.
The American Health Act ( AHA)
( - from Obama Care to Trump Care )
If agreed to - by Mr. Trump: On May 31, 2017, the American Health Act [ AHA ] shall be introduced by the Donald J. Trump Presidential Administration. The AHA (Act) shall be passed unanimously by the US Congress and receive a Presidential signature - within 2 business days.
President Franklin D. Roosvelt passed such sweeping legislation - during his presidency - And, similar to today - the times and the conditions warranted this.
https://millercenter.org/president/fdroosevelt/domestic-affairs
Key features of the AHA:
- The primary objective of the Act is to protect, promote and restore the physical and mental well-being of citizens of the USA - and, to facilitate reasonable access to health services - through out America - without financial, physical or other barriers. We are all Americans. And, America is a great country. This ACT takes a step to re-claim our international heritage - as a world-leader in all things.
- Another objective of the American Health Act is: continued access to quality health care - without financial or other barriers - for all Americans; as this will be critical to maintaining and improving the health and well-being of all Americans - during any transition from "Obama Care" to "Trump Care".
- To do so, the AHA shall list a set of criteria and conditions (drafted below) that each state - in our Union of 50 States - must follow in order to receive Federal Transfer Payments ( FTPs ). They are - briefly: A) Public Administration - by States, B) Comprehensiveness & Universality, C)Portability, D) Accessibility - and E) Penalties.
- Additional criteria and conditions - extending and altering this AHA - may be introduced into the US Congress (after May 31, 2017) for voting upon by the elected representatives of the American people - as conditions and experience - with the enacted AHA - warrant.
The criteria & conditions - to be met by each state AHA provider are as follows:
A) Public administration
- All AHA medical and health related services and entities must be "administered" and "operated" on a non-profit basis by licensed Medical Professionals - responsible (only) to US State governments and their medical peers.
- The "entities" administered and operated are subject to audits of their records, accounts and financial transactions - by State Government and AHA officials.
- Elimination: All so-called and in reality "Private Insurance Companies & Carriers" shall be eliminated (by this ACT) - until time and experience provides sufficient proof they are necessary - for any practical reason. That is, no one should benefit from the pain and suffering - of an American citizen.
- An ACT of the US Congress - shall be necessary to reverse the previous provision of "elimination".
B) Comprehensiveness & Universality
- There shall be no such entity - in the United States of America - as a "non-insured citizen".
- That is, every United States citizen (born and living) shall be covered and cared for - by reasonably re-numerated Medical Professionals.
- All AHA services shall be provided in excellent "World Class" American Medical Facilities - as required and needed - with no apportionment - related to a State's individual wealth or population.
- The AHA shall cover all health services provided by Medical Professionals in these facilities ( in every state) - including (as needed) psychiatry and dentistry.
- The fees (for AHA services) that may be charged - by Medical Professionals - are as described and stated in the current published USA Medicare program documents (2017).
- If Medical Professionals wish to offer services - that are not currently described by USA Medicare program documents - they may do so; however, those "additional services" shall be provided on a private business basis - and, not covered or administered by the AHA; however, all FDA & USHHS rules and regulations shall apply & be enforced.
- No Medical Professional (employed to provide services - under the AHA) - shall be permitted to simultaneously provide private business services.
- The states are permitted, to offer additional "distinguishing" medical and dental services; however, these "additional services" shall be paid for exclusively by State Transfer Payments (STPs). These STPs shall be administered by the States - and, they may not be made fungible - or, made a part of the AHA ( FTP) funds - in any manner.
C) Portability
- States shall be responsible for their state citizens - who are temporarily in another state - for purposes of work, travel, visiting, etc.
- "Temporary" from more "permanent" relocation status shall be determined - using 90 days as a standard maximum - to make the distinction ( of permanent versus temporary resident) at the program's start.
D) Accessibility
- The AHA shall provide Medical Professionals with the means to provide uniform "reasonable access" to services offered for USA citizens - using all modes of public USA transportation systems ( including trains, plains, buses, taxis, etc.) on uniform terms and conditions.
- Medical Professionals ( after licensure) shall be at liberty to "move about" in America - and, subsequently licensed in other US states.
- All AHA services shall be provided in similar and comparable "World Class" medical facilities - located in every state in America.
- There shall be no "extra-billing" - of any American citizen - for any AHA services rendered.
- Specifically, Medical Professionals in every American location - which, they choose to be located in - shall be re-numerated - at the same AHA rate (per specialty) - adjusted only for provable State "cost-of-living" differences - which, are not "controllable" by other means - such as, medical facility offerings. ( For example, AHA Medical Facilities may provide Medical Professional dormitories, meal rooms, laundries etc.)
- AHA Medical Professional day-to-day travel expenses shall not be reimbursed - through AHA funds. This is to encourage employed AHA Medical Professionals, to live near - where they choose to work - which, will result in improved inner-city areas.
E) Penalties
- The states shall ensure recognition of the Federal Transfer Payments ( FTPs) by publically viewable documents - modeled after modern transaction receipts (on state web sites, etc.)
- States shall provide information to appointed AHA officers as requested. The AHA shall mandate a Director - with staff.
- The size and scope of the AHA "directorate" shall dictate its annual budget.
- The AHA Federally designated Director and their "staff" is entitled to request and receive specific information related to a state's AHA health care services.
- This "information" shall be used in drafting AHA annual reports ( to Congress) - which shall be made available and presented to the American people - regarding how each state has administered its AHA health care services over the previous year.
- This information shall be provided on a timely basis (to the AHA staff) - on a level of detail - as requested by the AHA Federally designated "staff".
- The AHA "Director" shall be appointed by the current President of the United States (during her or his term) - and, no confirmation ( by the US Congress ) is required.
- Each AHA Director ( so named ) - shall offer their resignation - at the end of the "appointing President's" term.
- Each state must "give recognition" to the USA federal government ( as the "ultimate provider" of AHA services ) in public documents and in any advertising or promotional material, relating to Federal AHA health services in the state.
- For non-compliance - with any of the criteria listed above - the federal government ( upon proof) shall withhold all or a part of the Federal Transfer Payment.
- The federal government shall actively enforce these criteria - utilizing all eligible enforcement capabilities of its departments: DOJ, etc.
- Specifically, in recognition of the "status", "privilege" and "honor" that American society confers on licensed Medical Professionals, no Medical Professional shall a) organize "unions" or b) go on "strike" - or, c) take actions to undermine the intent of the AHA - without risk to their State and Federally granted medical license.
[ end of idea ]
A Curator's Look at the House Chamber :: In this video, House Curator Farar Elliott paints a picture of what the Chamber looked like long ago, and how it looks today.
Direct Link:
http://history.house.gov/Media?mediaID=41347
https://www.fsmb.org/Media/Default/PDF/Census/2014census.pdf
Physicians with "active" license - to practice medicine = 812, 019 (Table 1)
The current United States Population - 4-8-2017 = 325,933,992
http://www.worldometers.info/world-population/us-population
2017-2018 (115th Congress)
|
https://rules.house.gov < web site
https://rules.house.gov/committee-rules-members ( shown below )
https://rules.house.gov/bill/115/hr-1628 American Health Care Act of 2017
- current information
https://rules.house.gov/amendments ( Where & HOW to submit amendments to any official Bill.)
- Hon. Louise McIntosh Slaughter - Ranking Minority Member - New York: https://louise.house.gov
Hon. James P. McGovern - Massachusetts: http://mcgovern.house.gov
Hon. Alcee L. Hastings - Florida: http://alceehastings.house.gov
Hon. Jared Polis – Colorado: https://polis.house.gov
Hon. Pete Sessions – Chairman – Texas:
https://sessions.house.gov
1275
https://www.congress.gov/bill/115th-congress/house-bill/1275/text
Hon. Tom Cole - Vice-Chairman, - Oklahoma: https://cole.house.gov
Hon. Rob Woodall – Georgia: https://woodall.house.gov
Hon. Michael C. Burgess – Texas: https://burgess.house.gov
Hon. Doug Collins – Georgia
https://dougcollins.house.gov
Hon. Bradley Byrne - Alabama
https://byrne.house.gov
Hon. Dan Newhouse – Washington
https://newhouse.house.gov
Hon. Ken Buck - Colorado: https://buck.house.gov
Hon. Liz Cheney – Wyoming:
https://cheney.house.gov
Health (Ways & Means)
(https://waysandmeans.house.gov)
Republican Members
Michael Burgess (Texas - 26)
- Chairman
Brett Guthrie (Kentucky - 02)
- Vice Chairman
Joe Barton (Texas - 06)
Fred Upton (Michigan - 06)
John Shimkus (Illinois - 15)
Tim Murphy (Pennsylvania - 18)
Marsha Blackburn (Tennessee - 07)
Cathy McMorris Rodgers (Washington - 05)
Leonard Lance (New Jersey - 07)
Morgan Griffith (Virginia - 09)
Gus Bilirakis (Florida - 12)
Billy Long (Missouri - 07)
Larry Bucshon (Indiana - 08)
Susan Brooks (Indiana - 05)
Markwayne Mullin (Oklahoma - 02)
Richard Hudson (North Carolina - 08)
Chris Collins (New York - 27)
Buddy Carter (Georgia - 01)
Greg Walden (Oregon - 02) - Ex Officio
Members
Gene Green (Texas - 29)
- Ranking Member
Eliot Engel (New York - 16)
Janice Schakowsky (Illinois - 09)
G. K. Butterfield (North Carolina - 01)
Doris Matsui (California - 06)
Kathy Castor (Florida - 14)
John Sarbanes (Maryland - 03)
Ben Lujan (New Mexico - 03)
Kurt Schrader (Oregon - 05)
Joseph P. Kennedy III (Massachusetts - 04)
Tony Cárdenas (California - 29)
Anna Eshoo (California - 18)
Diana DeGette (Colorado - 01)
Frank Pallone (New Jersey - 06)
Pat Tiberi (OH)
Sam Johnson (TX)
Devin Nunes (CA)
Peter Roskam (IL)
Vern Buchanan (FL)
Adrian Smith (NE)
Lynn Jenkins (KS)
Kenny Marchant (TX)
Diane Black (TN)
Erik Paulsen (MN)
Tom Reed (NY)
Minority
Sander Levin (MI)Mike Thompson (CA)
Ron Kind (WI)
Earl Blumenauer (OR)
Brian Higgins (NY)
Terri Sewell (AL)
Judy Chu (CA)
|
|
|
|
|
Added 4-6-2016 [ Thank you! to Mr. Jon E. for your review and comments - on my 4-4-2017 draft ]
Life - Liberty and the Pursuit of Happiness ("unalienable rights" & US Health Care)
"Life, Liberty and the pursuit of Happiness" is a well-known phrase in the United States Declaration of Independence. (1776). The phrase gives three examples of the "unalienable rights" which the Declaration says have been given to all human beings by their "Creator", and which governments are created to protect. The first US citizens fought and died to protect and defend their inalienable rights.
Clearly, US Health Care related laws and government policy - directly effects every US citizen's life, liberty and happiness. Thus, any laws - enacted in this area - would find their origin in penumbral rights and US History - as the word "health" cannot be found in the [current] US Constitution - or, its amendments.
" Typically, the term un-enumerated rights describes certain fundamental rights that have been recognized by the U.S. Supreme Court under the U.S. Constitution. In addition, state courts have recognized un-enumerated rights emanating from the principles enunciated by their own state constitutions. No comprehensive list of un-enumerated rights has ever been compiled nor could such a list be readily produced precisely because these rights are un-enumerated." ( http://legal-dictionary.thefreedictionary.com/Unenumerated+Rights : 4-6-2017 )
"Penumbral Rights" - in US Law [ https://en.wikipedia.org/wiki/Penumbra_(law) ]
In science, a penumbra is the partial or imperfect shadow outside the complete shadow of an opaque body. For example: a planet, where the light from the source of illumination (a Sun) is only partly cut off - that is, a shadowy, indefinite, or marginal area - then exists. Or, hold your hand in front of a light bulb - and look momentarily. You will see a penumbra. Comparatively, an "umbra" is the complete or perfect shadow cast by an opaque body. For example, a planetary body - where the direct light from the source of illumination is completely cut off. That is, there is no shadowy, indefinite, or marginal area. The earth's moon experiences an umbra during a "total lunar eclipse" event.
A strict interpretation of the US Constitution - would not permit "penumbras" to exist ( in law) or take effect - unless they were "fair". Antonin Gregory Scalia, an Associate Justice - of the Supreme Court of the United States (from 1986 until his death in 2016) was most identified with the term "strict interpretation" and "constructionist". Justice Scalia summarized his textualist approach as follows: "A text should not be construed strictly, and it should not be construed leniently; (a text) should be construed reasonably, to contain all that it fairly means."
In United States constitutional law, the "penumbral rights" include a group of rights derived, by implication, from other rights explicitly protected in the US "Bill of Rights". Penumbral rights ( for US citizens ) have been identified through a process of "reasoning-by-interpolation", where specific principles are recognized from "general ideas" that are explicitly expressed in other constitutional provisions.
Although researchers have traced the origin of the term ( penumbra ) to the nineteenth century, the term first gained significant popular attention in 1965, when Justice William O. Douglas's majority opinion in Griswold v. Connecticut identified a right to privacy in the penumbra of the constitution.
The "Bill of Rights" is the first ten amendments to the United States Constitution. The US Bill of Rights (aka "amendments 1 through 10") were added to the US Constitution ( that was ratified by then States in 1788). That is, specific guarantees of personal freedoms and rights, clear limitations on the government's power in judicial and other proceedings, and explicit declarations that all powers not specifically delegated to Congress by the Constitution are reserved for the states or the people.
The Bill of Rights "additions" ( first suggested by James Madison ) became Amendments One through Ten of the US Constitution ( on December 15, 1791). The majority of the seventeen later amendments ( to the US Constitution) expand individual civil rights protections. Others relate to federal authority or modify government processes and procedures.
|
|
---- hhhhhhhhhhhhhhhhhhhhhhhh
hhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhh
Hhhfrom Susan’s web site hhhhhhhhhhhhhhhhhhhh
hhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhh
Again, I say "THANK YOU".
Your grateful constituent - Mrs. Susan Marie CASSADY-Neuhart
http://www.cnbc.com/2017/05/04/look-at-how-your-congressman-voted-on-the-republican-obamacare-replacement-bill.html
The Republican bill [HR1628]... to repeal and replace major parts of Obamacare drew 217 "yes" votes in the House, and 213 "no" votes on Thursday 5-4-2017.
All 193 Democrats voting on the American Health Care Act opposed it. They were joined by 20 Republicans - AND, one of them was Mr. Mike Turner [ H-10 ]
Click here to see how your member of Congress voted> http://clerk.house.gov/evs/2017/roll256.xml < Official "clerk's report
H R 1628 ( RECORDED VOTE) 4-May-2017 @ 2:18 PM - BILL TITLE: American Health Care Act ---- NOES 213 ---
Hhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhh
|
http://thedailyvoicenews.com/2017/05/05/how-ohio-representatives-voted-on-the-ahca
How Ohio Representatives Voted ... (AHCA-1628) May 4, 2017
There are 16 USA Con. districts in Ohio.
The following is the official roll call of votes on the American Health Care Act by Ohio...
Rep. Steve Chabot, Republican: Voted Yes
Rep. Brad Wenstrup, Republican: Voted Yes
Rep. Joyce Beatty, Democrat: Voted No
Rep. Jim Jordan, Republican: Voted Yes
Rep. Robert Latta, Republican: Voted Yes
Rep. Bill Johnson, Republican: Voted Yes
Rep. Bob Gibbs, Republican: Voted Yes
Rep. Warren Davidson, Repub. : Voted Yes
Rep. Marcy Kaptur, Democrat, Voted No
Rep. Michael Turner, REP. -Voted NO
Rep. Marcia Fudge, Democrat: Voted No
Rep. Patrick Tiberi, Republican: Voted Yes
Rep. Tim Ryan, Democrat: Voted No
Rep. David Joyce, REP. : Voted NO 1,2,3,4
Rep. Steve Stivers, Republican: Voted Yes
Rep. James Renacci, Republican: Voted Yes
|
|
|
|
|
H & C
H&C
H&C H&C
Hhhhhhhhhhhhhhhhhhhhhhhh
|
https://www.democraticunderground.com/index.php < DEMOCRATIC UNDERGROUND!
 ONE of the nicest things my daughter ever said to me: "Mom, she's like you." (Dawn had related (to me) an incident [ she witnessed] - while serving on Capital Hill. She was present ( she stated) - in a meeting - during the early 1990s; Where, a person - in the meeting ( with Maxine Waters ) - started to shove "a small toy baby doll" - at her [Congresswoman Maxine Waters]. Maxine stopped the "shove" - gently. Took hold of the toy doll. And then, shoved it ( "gently" ) right - back - at the person - and, made a quite statement. That my daughter - thought was most appropriate. I am ( like most American women ) a great "admirer of Ms. Waters. So, to be "compared" - to her - by my daughter - was, a tremendous compliment. Ms. Waters represents an American "Profile() of Courage" - that women [ all over the world ] need to be aware of. Moreover, American women are safer (today) - because of her efforts. Thank you! Ms. Waters - for your public service. (VAWA) ONE of the nicest things my daughter ever said to me: "Mom, she's like you." (Dawn had related (to me) an incident [ she witnessed] - while serving on Capital Hill. She was present ( she stated) - in a meeting - during the early 1990s; Where, a person - in the meeting ( with Maxine Waters ) - started to shove "a small toy baby doll" - at her [Congresswoman Maxine Waters]. Maxine stopped the "shove" - gently. Took hold of the toy doll. And then, shoved it ( "gently" ) right - back - at the person - and, made a quite statement. That my daughter - thought was most appropriate. I am ( like most American women ) a great "admirer of Ms. Waters. So, to be "compared" - to her - by my daughter - was, a tremendous compliment. Ms. Waters represents an American "Profile() of Courage" - that women [ all over the world ] need to be aware of. Moreover, American women are safer (today) - because of her efforts. Thank you! Ms. Waters - for your public service. (VAWA)
Thus, America is better - because of :
A) "Public Schools" (The University of Wisconsin [UWGB] is a "public" education institution). And, all - but $6,000 - of my higher-education costs ( circa 1977 - 1982) were covered by USA DOE Education - grants and "Work-Study" programs.
B) And, America is stronger & safer [F35-JSF] - because, my daughter was employed (by me) - in a "high-tech" independent business venture - where she daily (was required) - related to her duties as a textbook "digital artist" - to study and absorb - Science Technology Engineering & Math [STEM];
C) and, Dawn was [thus] very able & capable to play a very significant role - in the:
a) creation of the "Unmatched" - by any other country in the world: F35 Joint-Strike-Fighter air craft...
b) AND, the re-election (several times) of the Honorable Mr. John Conyers to the United States Congress.
[ https://en.wikipedia.org/wiki/John_Conyers ]
D) And, America will be much more improved & "returned" to Greatness instantly - if the US Congress (under Paul Ryan's leadership ) - passes a "Universal Health CARE ACT" [HR 676] - for President Trump's approval.
YES! Friends - God does work in mysterious ways! And, she always has! Please support! Mr. John Conyer's (now) fully sponsored HealthCARE legislation [hr676]; AND, May God and - his son - [Jesus Christ] continue to grace America, our "Public Schools" - and, Congressman John Conyers. ( Please see continuing research topics below.)
|
|
Medical doctors and the NEW Racism : http://www.alternet.org/personal-health/medical-racism-and-ignoring-black-pain < Copyrighted material 5-5-2017 !
|
|
https://waters.house.gov/ < Congress Woman Maxine Waters < "Hero!" Thank YOU! Maxine ( Ms. Waters )
|
|
|
|
|
|
|
|
|
|
|
( HR 676 ) < At the request of Congressman John Conyer's representatives... AND, other USA DEMOCRATS ( the above WWW information is provided - on a volunteer & Free-of-Charge basis - by Susan Marie Neuhart-CASSADY)
https://www.congress.gov/bill/115th-congress/house-bill/676
http://www.washingtonpost.com/wp-srv/politics/special/clinton/stories/conyers101398.htm
hhhhhhhhhhhhhhhhhhhhhhhhhhhhh
Dear Congressman Turner - Republican [ OH 10 ] , THANK YOU!
-- for your public service ( for Ohio 10th Congressional District! ) ( edited 5-4-2017 )
Sir, as you will recall, I am supportive of your efforts to make America & zip code 45405 a great place to live. And, it is already pretty nice.
Formerly, of Central Ohio - I now make my home in your Congressional district [ Ohio 10 ].
Specifically, I am not employed - or, paid - by YOU ( or anyone) - to say - or request - the following things:
MIKE (and you may call me "Susan") - PLEASE CO-SPONSOR HR 676
- being presented (again) by America's USA Congressman Mr. John Conyers. 13th District, Detroit, Michigan
The Co-Sponsors are listed on Mr. Conyer's Official USA Congressional web site.
:: https://www.congress.gov/bill/115th-congress/house-bill/676/cosponsors I hope to see you - and Mr. Trump - on that list soon. Current OHiO Co-sponsors 5-4-2017
There are good business reasons for my request - which, I present below - and ABOVE ****
Mr. Conyers ( see link above ) is the U.S. Representative for Michigan's 13th congressional district.
He has been a member of Congress since 1965; and, he is currently our Congress's longest-serving current member,
making him the "Dean of the House of Representatives."
As he may recall, Mr. Conyers - employed the services of my daughter ( Dawn Marie Burton) during his 1990-ish RE-election campaigns. He won!
[ In fact, I treasure the memory of Mr. Conyers - telephoning me at my business address - in 1990+ - and thanking me
- for sending (to him) my daughter. To work on his campaign. I chuckle (now) - for, in fact, I had done no such thing.
No!, my daughter had arranged that "gig" - all by herself.
It was only later - that I came to fully understand completely "who" and "what" John Conyers was. That is, a great human-being!
I knew - by the sound of his voice - He was famous - that - it was - "THE" John Conyers.
I recall he told me (that day): "Mom, you do not have to worry about your girl. I will take care of her." And, he did.
**** Sir, I was a small-business owner (in Central Ohio) for many years - and, during this time - one of my largest monthly expenses was
Health-Care coverage ( Blue-Cross/ Blue Shield ) for my employees. As you are aware (today) - my competitors ( many in other countries )
did not - and, do NOT have this cost. Thus, the expansion of MEDI-care - as proposed by Congressman Conyer's Bill [ HR 676 ] - would be a tremendous assistance to the Small-Business enterprises - of America.
In fact, the progress of this HR 676 - would: 1) Bring America into the mainstream of GREAT Country's that offer this - as a right - for their citizens [ the passage - of this alone - would help MAKE AMERICA GREAT AGAIN! ]; 2) place a huge benefit in the hands of America's small business owners AND their employees; and, 3) cover the American citizen - with Universal Health Insurance - in a manner that was first proposed - by President Harry Truman - at the request of FDR.
Sir, I am updating my web site with the "historical perspectives" of "American Universal Health Care" - since, the late 1800s - at this time.
I will soon be able to articulate - based on my research - WHO the "progressives" truly are - and, who and "why" the very notion - of "Socialized Medicine" - has powerful enemies.
Please GOOGLE to find my site: Susan Marie Cassady American Health :: I try to work on my site daily.
However, ( I admit) that I am slow - mostly, related to the stroke that I suffered. Not to worry - my doctors - who I am grateful for
- THEY think that I am doing good.
In fact, I am "carrying the flag" - for my medical doctors - on Health CARE - because, they feel, they may be out-cast... if they try to.
Again, (Mike) I will support YOUR efforts - as I am able to.
And, YOU & Mr. Trump [teamed-Up] - just may be able to succeed - at "Universal Health Care Reform" - where others - many others - have failed. (for over 100 years.)
I know that Mr. Trump would have the support of the "Dean" of the Democrats ( John Conyers). I think - together - we can get Ms. Pelosi on board - also.
Specifically, Mr. Trump does not "need" the AMA support; whereas, others - even past Presidents - according to my historical research (thus far) - were literally forced to pander to them. The historical roots of this will be presented on my web site.
Good Luck Sir! And, God's speed. - Susan
[ END ]
The historical roots of the AMA
the "historical perspectives" of the "American Universal Health Care" idea - since, the late 1800s -
**************************************
YES, Susan is still researching - and puzzled - and writing...
- as to WHY? American Health CARE - as a universal "right" - ( similar to "public education" ) - is so difficult - in the USA ?
Still researching... AND, Thank YOU! I am glad (that) you asked ...
http://www.pnhp.org/facts/a-brief-history-universal-health-care-efforts-in-the-us <<< A Brief History "Presentation" beginning
The following subjects - will be hyperlinked, investigated - read by "me" - and, referenced - in my forth-coming document
- in support of American Universal Health CARE efforts aka "socialized medicine".
That is, never shrink from a fight - but, do try to get them to come to "your ground" - to engage the enemy. https://www.churchillcentral.com/quotes
"Penumbra" and "implied rights" https://en.wikipedia.org/wiki/Penumbra_(law)
" Health Care" and "life, liberty & the pursuit ..." draft done
https://en.wikipedia.org/wiki/History_of_insurance
https://depts.washington.edu/bioethx/
AMA Physician Masterfile
https://www.ama-assn.org/life-career/ama-physician-masterfile
Congressional Salary & Benefits
https://www.senate.gov/CRSpubs/9c14ec69-c4e4-4bd8-8953-f73daa1640e4.pdf
Bernie Sanders Health Plan
https://berniesanders.com/medicareforall/
April_19_1775 < what happened?
http://www.history.com/this-day-in-history/the-american-revolution-begins
Physician Specialty dataBook ( 2014 )
https://members.aamc.org/eweb/DynamicPage.aspx?Action=Add&ObjectKeyFrom=1A83491A-9853-4C87-86A4-F7D95601C2E2&WebCode=ProdDetailAdd&DoNotSave=yes&ParentObject=CentralizedOrderEntry&ParentDataObject=Invoice%20Detail&ivd_formkey=69202792-63d7-4ba2-bf4e-a0da41270555&ivd_prc_prd_key=41FEE42C-6D95-4E8D-AC8A-1173945902A4
logic
Common-Sense - Thomas paine
https://www.law.gmu.edu/assets/files/academics/founders/Paine_CommonSense.pdf
Oaths-Medical Graduates
https://en.wikipedia.org/wiki/Hippocratic_Oath
Medical Schools – USA
https://en.wikipedia.org/wiki/List_of_medical_schools_in_the_United_States
Mr. Fred Strahorn Ohio STATE - district 39 :: https://en.wikipedia.org/wiki/Fred_Strahorn < https://en.wikipedia.org/wiki/Ohio_General_Assembly
Mr. Mike Turner [OH-10] - District Map < MY USA CONGRESSMAN
MICRA - manual PDF
https://en.wikipedia.org/wiki/Medical_Injury_Compensation_Reform_Act
Frontline2001_medMALpractice
http://www.pbs.org/wgbh/pages/frontline/health-science-technology/2.html
Medical MALpractice CRS 2 versions
"Life Settlements" US SEC
Medical Malpractice 2004 Wm Sage
The marketing of Insurance NAIC
Medical Malpractice Insurance Report
Insurance Times
WikiLeaks ( what is it ?) A prescription for Chaos https://books.google.com/books/about/Medical_Malpractice_Insurance.html?id=rKzxHAAACAAJ
Medical Malpractice insurance Report (9-2004)
Eric Nordman
The Social Security Act (the Act) requires the Centers for Medicare & Medicaid Services (CMS) to establish payments under the Medicare Physician Payment Schedule based on national uniform relative value units (RVUs) that account for the relative resources used in furnishing a service.
The Act requires that RVUs be established for 3 categories of resources:
1. Physician work
2. Practice expense (PE)
3. Malpractice (MP) expense
https://www.cms.gov/ < the Centers for Medicare & Medicaid Services
https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/DataCompendium/2011_Data_Compendium.html
Medicare Physician Fee Schedule
http://www.aafp.org/news/government-medicine/20161104finalmpfs.html
Defensive Medicine
https://en.wikipedia.org/wiki/Defensive_medicine
Duty < term of legal art : Google
requisite doctor-patient relationship is established
http://journalofethics.ama-assn.org/2012/05/hlaw1-1205.html
http://journalofethics.ama-assn.org
http://journalofethics.ama-assn.org/site/about.html
“reasonably competent physician” < term of legal art : Google
[1]
��Congressional Research Service (REPORT) AKA - "Medical Malpractice Insurance - A Prescription for CHAOS"
[ http://www.gjsentinel.com/news/articles/coloradocare-a-prescription-for-chaos ] <
blog by Rick Wagner > http://www.gjsentinel.com/staff/detail/58/
“ Insurance is a critical piece of a modern economic system, but it often goes unnoticed until it becomes prohibitively expensive or its availability is curtailed. Such problems reportedly occurred recently in the medical malpractice insurance market.
Many physicians experienced substantial increases in insurance premiums, and there have been reports of problems with availability of physician services due to doctors retiring or relocating from areas that have seen high premium increases. This was not the first time such a crisis has been proclaimed; similar events occurred in the latter half of both the 1970s and 1980s.
The fundamental purpose of insurance is to transfer an indefinite risk from one party to another for a definite premium. The pricing of this premium is critical, but determining this price is uncertain because it depends on estimates of the chance of a future loss, as well as the estimated value of that loss. The premium will also depend on estimates of future investment gains or losses because an insurer also acts as a financial intermediary and invests the capital that is held in reserve against future losses. “
Offering liability insurance for medical malpractice has proven a difficult market for insurance companies for a variety of reasons and the market has been unstable during the past three decades.
The recurring market problems have provoked various policy reactions in both state legislatures and in Congress.
Assessing the effectiveness of particular policy changes is, however, complex and strong conclusions have typically been equally strongly disputed.
In the 109th Congress, the House passed a bill, H.R. 5, whose centerpiece was a limitation on tort claims for medical malpractice; similar bills passed the House in the previous two Congresses.
The Senate, however, did not act on any of these House bills, and failed to invoke cloture on the Senate bills addressing medical malpractice.
There has been no floor or committee action on bills addressing medical malpractice issues in the 110th Congress.
This report examines the economic issues and historical experience surrounding medical malpractice insurance.
It includes an explanation of the fundamentals of insurance and how these fundamentals relate specifically to medical malpractice insurance.
It also includes a discussion of the evolution of the medical malpractice insurance market since the 1970s and policy changes over this time, including an assessment of these changes.
It will be updated as major legislative events occur but will not attempt to track legislation in detail.
*******************************************************
Hhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhh
6-25-2017
https://www.budget.senate.gov/about/committee-members
https://www.cbo.gov/publication/52752
https://www.cbo.gov/system/files/115th-congress-2017-2018/costestimate/hr1628aspassed.pdf
https://www.cbo.gov/topics/health-care
https://www.budget.senate.gov/about/committee-members
https://www.budget.senate.gov/bettercare
hhhhhhhhhhhhhhhhhhhhhh
Thursday, June 22
Statement by Senator Portman on Senate Health Care Discussion Draft
Portman issued the following statement on the discussion draft of the Senate health care legislation:
“As I’ve said previously, the Affordable Care Act is not working for many Ohio families and small businesses. My goal is to create a more workable system that lowers the cost of coverage, provides access to quality care, and protects the most vulnerable in our society. There are some promising changes to reduce premiums in the individual insurance market, but I continue to have real concerns about the Medicaid policies in this bill, especially those that impact drug treatment at a time when Ohio is facing an opioid epidemic.
“I look forward to examining this new proposal carefully and reviewing the analysis by the Congressional Budget Office when it is available. If the final legislation is good for Ohio, I will support it. If not, I will oppose it. As this process moves forward, I will continue to work to protect Ohio’s interests and ensure that our health care system works better for all Ohioans.”
hhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhhh
ALERT! The AMA document "AMA VISION ON HEALTH REFORM "- that I just "downloaded" is a sham - that ONLY (really) supports USA 'Health Insurance' companies - and, even more injustice!
Susan says: THE " AMA "IS Single-Payer Health Care's" ENEMY - (thus) "AMA" is "our"ENEMY! Please become informed. Inform any Medical Professionals (that you know) - and VOTE! [ Politics RNC & DNC ] Also - Let Us "protest" [if needed] - real nice & peaceful - like Dr. Martin Luther King (taught us to do) - if we have to!
( Susan's independently developed support DOC [ FOR " USA single-payer Health CARE" - still in progress. When ready, that PDF will be posted here [on my personal web site] ... ) till then> current researchNOTES
YES! You may use my hyperlinked notes, research, etc. & make your own document (or)... Please! - I urge everyone - only do USA "lawful" things.
"Never thinking a thing wrong - don't make it right." < Susan Marie CASSADY-Neuhart [ after Ms. Zora Neale Hurston ] < © 2017 - all rights reserved (by Susan)
Googled by Susan - 6-27-2017 : ( No results found for "Never thinking a thing wrong - don't make it right.". )
RESULT: https://www.google.com/search?q=%22Never+thinking+a+thing+wrong+-+don%27t+make+it+right.%22&rlz=1C1CHZL_enUS743US743&oq=%22Never+thinking+a+thing+wrong+-+don%27t+make+it+right.%22&aqs=chrome..69i57.2591j0j8&sourceid=chrome&ie=UTF-8
Also see: “A long habit of not thinking a thing wrong, gives it a superficial appearance of being right, and raises at first a formidable outcry in defense of custom.
But the tumult soon subsides. Time makes more converts than reason.” < Thomas Paine
[ Current END of page date: 7-15-2017 ]